| International Journal of Clinical Pediatrics, ISSN 1927-1255 print, 1927-1263 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Int J Clin Pediatr and Elmer Press Inc |
| Journal website https://ijcp.elmerpub.com |
Review
Volume 15, Number 2, June 2026, pages 37-50

Wearable Devices in Pediatric Obesity: A Comprehensive Review of Current Applications and Future Directions
Jyothi Ranga Patria, b, c, d, e, i ![]() , Vignesh Gunasekaranf
, Vignesh Gunasekaranf ![]() , Shravan Gangulag, Venkata Sushma Chamarthih
, Shravan Gangulag, Venkata Sushma Chamarthih ![]()
aHeritage Valley Family Medicine Residency Program, Beaver Falls, PA, USA
bUniversity of Pittsburgh, Pittsburgh, PA, USA
cLECOM, Erie, PA, USA
dPCOM, Philadelphia, PA, USA
eDuquesne University College of Medicine, Pittsburgh, PA, USA
fWVU Medicine, Martinsburg, WV, USA
gCoffeyville Regional Medical Center, Coffeyville, KS, USA
hValley Children’s Hospital, Madera, CA, USA
iCorresponding Author: Jyothi Ranga Patri, Heritage Valley Family Medicine Residency Program, Beaver Falls, PA, USA
Manuscript submitted February 26, 2026, accepted April 9, 2026, published online May 22, 2026
Short title: Wearables in Pediatric Obesity: Review and Future
doi: https://doi.org/10.14740/ijcp1051
| Abstract | ▴Top |
Pediatric obesity represents a critical global public health crisis affecting millions of children and adolescents worldwide. Traditional obesity interventions face significant challenges related to adherence, engagement, and long-term efficacy. Wearable devices have emerged as promising tools for monitoring physical activity, metabolic parameters, and supporting behavior change in youth with obesity. This targeted literature review examines the current scope, applications, and effectiveness of wearable devices in managing childhood and adolescent obesity. We conducted a targeted literature review using PubMed and Google Scholar databases to identify studies published between 2010 and 2025. Search terms included wearable devices, pediatric obesity, activity trackers, accelerometers, continuous glucose monitors (CGMs), smartwatches, children, and adolescents. We focused on randomized controlled trials, systematic reviews, meta-analyses, and observational studies evaluating wearable devices in pediatric populations with obesity or overweight. Wearable devices demonstrate significant potential across multiple domains in pediatric obesity management. Activity trackers and accelerometers show effectiveness in increasing physical activity and improving anthropometric outcomes including body mass index (BMI), BMI z-score, and body fat percentage. Consumer-grade devices like Fitbit and research-grade accelerometers have shown acceptable accuracy and feasibility in pediatric populations. CGMs are emerging as valuable tools for understanding glycemic variability and supporting dietary behavior change in youth with obesity. Heart rate monitors and smartwatches provide real-time biofeedback that enhances engagement. However, heterogeneity in device types, intervention duration, and outcome measures limits definitive conclusions. In conclusion, wearable devices represent a versatile and increasingly accessible approach to pediatric obesity management. While current evidence supports their use for physical activity promotion and metabolic monitoring, significant gaps remain regarding long-term adherence, optimal implementation strategies, and integration into clinical care pathways. Future research should focus on standardizing outcome measures, evaluating cost-effectiveness, and developing age-appropriate interventions that maximize the unique potential of wearable technology in combating the pediatric obesity epidemic.
Keywords: Wearable devices; Pediatric obesity; Activity trackers; Accelerometers; Continuous glucose monitoring; Physical activity; Digital health interventions; Health monitoring
| Introduction | ▴Top |
Pediatric obesity remains one of the defining public health challenges of our time. According to the World Obesity Federation, more than 250 million children and adolescents worldwide are projected to have obesity by 2025 [1]. This epidemic carries profound implications for both immediate and long-term health. Children with obesity face increased risks of cardiometabolic complications, type 2 diabetes mellitus, hypertension, dyslipidemia, and psychosocial consequences that persist into adulthood [2, 3].
Traditional approaches to pediatric obesity management rely heavily on behavioral lifestyle interventions targeting diet, physical activity, and sedentary behaviors [4]. However, these interventions often achieve only modest outcomes due to poor adherence, limited engagement, and the complex interplay of genetic, environmental, and socioeconomic factors [5]. The heterogeneous response to standard treatment protocols underscores the need for innovative strategies that can provide personalized, continuous support for weight management in young populations.
Wearable technology has revolutionized health monitoring across multiple domains over the past decade. These devices, which include activity trackers, accelerometers, pedometers, smartwatches, and biosensors, offer unique capabilities for objective measurement and real-time feedback [6]. Unlike traditional methods that rely on self-report or periodic clinic visits, wearables enable continuous data collection in free-living conditions. This creates opportunities for precision medicine approaches tailored to individual patterns and needs.
The appeal of wearable devices for pediatric populations is particularly compelling. Today’s children and adolescents have grown up as digital natives, demonstrating high comfort levels with technology [7]. Wearables can leverage gamification, social connectivity, and immediate feedback mechanisms that resonate with youth culture. However, questions remain about the actual effectiveness of these devices in achieving meaningful health outcomes, their accuracy in pediatric populations, and optimal strategies for implementation.
Several systematic reviews have examined wearable devices in adult obesity populations, demonstrating improvements in physical activity levels and anthropometric outcomes [8, 9]. Yet until recently, comprehensive evaluations specific to children and adolescents remained limited. The physiological differences between adults and youth, including growth patterns, developmental stages, and distinct movement behaviors, necessitate separate evaluation of wearable technology performance in pediatric cohorts.
This review examines the current landscape of wearable devices in pediatric obesity management. We synthesize evidence on device types, clinical applications, effectiveness for anthropometric and behavioral outcomes, feasibility and acceptability among youth, and integration into obesity treatment protocols. Understanding the scope and limitations of current wearable technology will inform both clinical practice and future research directions in addressing the pediatric obesity crisis.
| Materials and Methods | ▴Top |
Literature search strategy
We conducted a comprehensive literature review to identify relevant studies on wearable devices in pediatric obesity. Our search strategy targeted two major academic databases: PubMed and Google Scholar. The search covered publications from January 2010 to December 2025 to capture the evolving landscape of wearable technology applications. We selected PubMed and Google Scholar as our primary databases because PubMed provides comprehensive coverage of biomedical literature indexed in MEDLINE, while Google Scholar captures a broad range of multidisciplinary sources including grey literature and conference proceedings. We acknowledge that additional databases such as Embase, Cochrane Library, and Web of Science were not included, which may have limited identification of some relevant studies, particularly those published in non-biomedical technology journals. However, given the targeted nature of this review and the overlap in indexed content across databases, we believe that our search strategy captured the majority of the pertinent literature.
Search terms
We employed the following search terms and combinations: “wearable devices,” “activity trackers,” “fitness trackers,” “accelerometers,” “pedometers,” “smartwatches,” “continuous glucose monitor,” “heart rate monitor,” “pediatric obesity,” “childhood obesity,” “adolescent obesity,” “overweight children,” “physical activity,” and “weight management.” Boolean operators (AND, OR) were used to refine searches and capture relevant literature.
Inclusion criteria
Studies were included if they met the following criteria: 1) participants were children or adolescents aged 2 to 18 years; 2) study population included individuals with overweight or obesity, or general pediatric populations where wearable devices were evaluated for obesity prevention; 3) intervention or assessment involved wearable devices for measuring physical activity, metabolic parameters, or supporting behavior change; 4) outcomes included anthropometric measures (body mass index (BMI), BMI z-score, body weight, body fat percentage, waist circumference), physical activity metrics, or feasibility/acceptability data; 5) study designs included randomized controlled trials (RCTs), systematic reviews, meta-analyses, observational studies, or feasibility studies.
Exclusion criteria
We excluded studies that 1) focused exclusively on adult populations; 2) evaluated non-wearable digital interventions such as smartphone applications alone, video games, or social media platforms; 3) examined wearable devices for conditions other than obesity without obesity-related outcomes; 4) were published in languages other than English; 5) lacked sufficient methodological detail or outcome data.
Data extraction and synthesis
Given the heterogeneity of study designs, device types, and outcome measures, we employed a narrative synthesis approach. We extracted information on study characteristics, participant demographics, device types, intervention components, outcome measures, and key findings. Studies were organized thematically by device type and application domain to facilitate comprehensive understanding of the current evidence base. Two authors (JRP and VSC) independently screened titles and abstracts for eligibility. Discrepancies were resolved through discussion and consensus with a third author (VG).
| Types of Wearable Devices in Pediatric Obesity | ▴Top |
Activity trackers and accelerometers
Activity trackers and accelerometers represent the most extensively studied category of wearable devices in pediatric obesity research. These devices use motion sensors to detect and quantify physical movement, providing objective measurements of steps, distance traveled, active minutes, and energy expenditure [10].
Research-grade accelerometers, such as the ActiGraph GT3X and GT3X+, have been validated extensively in pediatric populations. These devices typically attach to the hip or wrist and record movement data at high temporal resolution [11]. Studies have demonstrated their utility in capturing sedentary behavior, light physical activity, and moderate-to-vigorous physical activity (MVPA) in children across various settings [12]. However, challenges exist in determining appropriate cut-points for different age groups and in accurately capturing certain activities like cycling or swimming.
Consumer-grade activity trackers, including Fitbit devices, Jawbone UP, and Garmin wearables, have gained widespread popularity. A validation study of the Fitbit Flex in preschool-aged children (3–5 years) found acceptable accuracy for measuring sedentary behavior and total physical activity, with classification accuracies (receiver operating characteristic–area under the curve (ROC–AUC)) of 0.92 for sedentary behavior and 0.92 for total physical activity [13]. The same study noted moderate performance for light physical activity (0.63) and MVPA (0.77), suggesting some limitations in intensity classification.
Pedometers offer a simpler but still valuable approach to physical activity monitoring by counting steps. Studies in children with obesity have shown that pedometers can accurately capture ambulatory activity, particularly walking and stair climbing [14]. Research suggests that boys should accumulate approximately 13,000 steps per day and girls approximately 12,000 steps per day to meet recommendations for 60 min of moderate physical activity [15].
Continuous glucose monitors (CGMs)
CGM technology has expanded beyond its traditional use in diabetes management to emerge as a novel tool in pediatric obesity research. These devices measure interstitial glucose concentrations continuously throughout the day and night, providing detailed insights into glycemic variability and metabolic responses to dietary intake and physical activity [16].
Recent studies have explored CGM use specifically in children and adolescents with obesity who do not have diabetes. A scoping review found that CGM devices are well-tolerated in pediatric obesity populations, with no unique safety concerns compared to other populations [17]. Studies typically employed CGM for relatively short periods (1–14 days) to characterize glucose metabolism and identify abnormalities.
Emerging evidence suggests that CGM may serve multiple roles in obesity management. First, it can identify prediabetes and glucose dysregulation in youth with severe obesity, where prevalence reaches approximately 13% [18]. Second, CGM provides real-time biofeedback that may facilitate dietary behavior change. A 6-week crossover trial found that when youth with obesity had access to real-time glucose data (unmasked CGM) versus blinded CGM, they demonstrated increased awareness of how food choices affected their glucose levels [19].
Intervention studies have begun testing whether CGM feedback can modify eating behaviors. A 12-week study examining high-protein breakfast consumption found that CGM documented statistically significant reductions in glycemic peaks and time spent above normal glucose range [20]. Another study evaluating time-restricted eating combined with CGM showed that 88% of participants had positive opinions about sensor use, suggesting high acceptability [21].
Key CGM metrics applicable to obesity research include time in range (TIR), time above range (TAR), glucose variability measures such as coefficient of variation, and AUC for glucose excursions. However, standardization of these metrics for non-diabetic populations remains an area requiring further investigation [22].
Heart rate monitors and smartwatches
Heart rate monitoring provides physiological data that complements motion-based activity tracking. Modern wearable devices increasingly incorporate optical heart rate sensors using photoplethysmography (PPG) technology. These sensors enable real-time heart rate measurement during various activities and can estimate exercise intensity zones [23].
Several studies have evaluated smartwatches with integrated heart rate monitoring in pediatric physical activity interventions. The Samsung Gear Fit, Apple Watch, Garmin Vivofit series, and Polar devices have been used in research and clinical settings [24]. These devices offer advantages of combining multiple sensors (accelerometer, heart rate, global positioning system (GPS)) in a single, socially acceptable form factor that children are more likely to wear consistently.
A study examining personalized tracking of physical activity in children using wearable heart rate monitors found that real-time heart rate data could be leveraged to create adaptive exercise games that automatically adjust difficulty based on the child’s physiological response [25]. This represents an innovative application where wearables enable truly personalized interventions.
Heart rate monitoring also helps address limitations of accelerometry-based devices. Activities that involve upper body movement, resistance training, or cycling may not generate sufficient accelerometer counts but will elevate heart rate appropriately. The combination of motion and cardiac data provides more comprehensive physical activity assessment [26].
Multi-sensor devices and emerging technologies
Advanced wearable systems combine multiple sensors to capture diverse physiological and behavioral data. Devices like the SenseWear armband integrate accelerometry, heat flux sensors, galvanic skin response, and skin temperature to estimate energy expenditure more accurately than single-sensor devices [27].
Emerging wearable technologies show promise for future applications. Wearable cameras can assess dietary intake and food environment exposures in real-world settings [6]. Smart clothing with embedded sensors can monitor respiration, muscle activity, and body position. Skin patch sensors may eventually enable continuous monitoring of metabolic biomarkers beyond glucose.
The rapid evolution of consumer wearable technology continues to expand possibilities. Current devices increasingly feature longer battery life, water resistance, smartphone connectivity, and sophisticated data analytics platforms. These advances improve feasibility for sustained use in pediatric populations. The classification and clinical applications of wearable devices in pediatric obesity management are outlined in Figure 1.
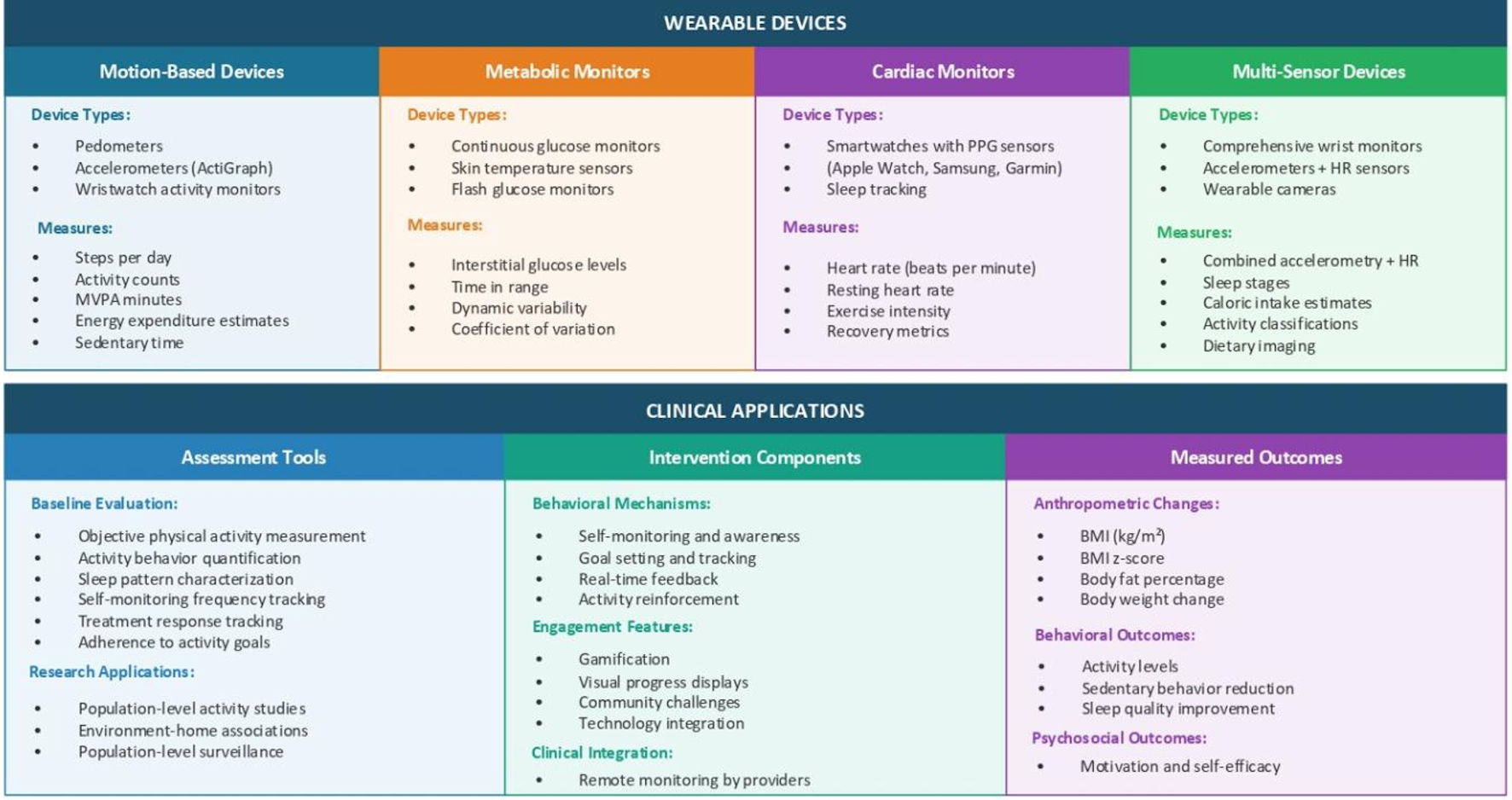 Click for large image | Figure 1. Classification and clinical applications of wearable devices in pediatric obesity management. This figure illustrates the four main categories of wearable devices used in pediatric obesity research and clinical practice. The top panel shows device classification: 1) motion-based devices including pedometers, accelerometers (ActiGraph), consumer trackers (Fitbit, Garmin), and wristband activity monitors, which measure steps per day, distance traveled, active minutes, MVPA duration, energy expenditure estimate, and sedentary time; 2) metabolic monitors including continuous glucose monitors (FreeStyle Libre, Dexcom), real-time CGM (RT-CGM), and flash glucose monitoring, which measure interstitial glucose levels, TIR, time above/below range, glycemic variability, glucose excursions, and coefficient of variation; 3) cardiac monitors including smartwatches with PPG sensors (Apple Watch, Samsung Galaxy), Polar HR monitors, and chest strap monitors, which measure HR (beats per minute), HR variability, resting HR, exercise intensity zones, cardio fitness score, and recovery metrics; 4) multi-sensor devices including SenseWear armband, ActiHeart, wearable cameras, and smart clothing/textiles, which combine accelerometry with HR, heat flux, galvanic skin response, skin temperature, sleep stages, and dietary imaging. The lower panel depicts clinical applications across three domains: 1) assessment tools (baseline evaluation including objective physical activity measurement, sedentary behavior quantification, and sleep pattern characterization; ongoing monitoring including treatment response tracking, adherence to activity goals, and real-world behavior patterns; research applications including intervention effectiveness studies, environmental factor associations, and population-level surveillance); 2) intervention components (behavioral mechanisms including self-monitoring and awareness, goal-setting and tracking, real-time feedback, and positive reinforcement; engagement features including gamification elements, social connectivity/challenges, visual progress displays, and achievement rewards; clinical integration including remote monitoring by providers); and 3) measured outcomes (anthropometric changes including BMI, BMI z-score, body fat percentage, body weight, and waist circumference; behavioral outcomes including physical activity levels, sedentary behavior reduction, and dietary awareness/modification; psychosocial outcomes including motivation and self-efficacy). MVPA: moderate-to-vigorous physical activity; PPG: photoplethysmography; TIR: time in range; HR: heart rate; BMI: body mass index. |
| Evidence for Effectiveness in Pediatric Obesity | ▴Top |
Impact on physical activity outcomes
A comprehensive systematic review and meta-analysis by Wang et al evaluated wearable devices as physical activity interventions for preventing and treating obesity in children and adolescents [28]. The review included 12 RCTs with over 3,000 participants aged 6 to 18 years. Devices used included pedometers (seven studies) and wristband activity trackers (five studies), with intervention durations ranging from 2.5 to 18 months.
The meta-analysis demonstrated statistically significant improvements in several anthropometric outcomes. Wearable device interventions resulted in significant reductions in BMI, BMI z-score, body fat percentage, and body weight compared to control groups. Effect sizes varied by outcome measure and study characteristics, but overall findings supported the effectiveness of wearables for obesity-related outcomes in youth.
A more recent systematic review and meta-analysis published in The Lancet Digital Health examined the effect of wearable activity trackers on physical activity in children and adolescents [29]. This review included 31 studies with 6,329 participants. Findings showed that wearable trackers significantly increased daily step counts, with participants accumulating on average 1,205 additional steps per day (95% confidence interval (CI): 626 to 1,784 steps). However, the devices did not significantly increase MVPA, suggesting that increased steps may not always translate to higher intensity exercise.
Subgroup analyses revealed important moderators of effectiveness. Interventions that included additional behavioral components (goal setting, feedback, rewards, education) showed stronger effects than wearables alone. Intervention duration also mattered, with optimal effects observed between 8 to 12 weeks. Effects tended to diminish over longer periods, highlighting challenges with sustained engagement.
Anthropometric outcomes
Evidence for wearable device interventions improving anthropometric measures shows promise but with heterogeneity across studies. The meta-analysis by Wang et al found the following pooled effect sizes: BMI (mean difference: –0.50 kg/m2, 95% CI: -0.90 to -0.11, p=0.01), BMI z-score (mean difference: –0.05; 95% CI, –0.09 to –0.01; P = 0.03), body fat percentage (mean difference: –1.14%; 95% CI, –2.17% to –0.11%; P = 0.03), and body weight (mean difference: –1.26 kg; 95% CI, –2.32 to –0.20 kg; P = 0.02) [6].
These effects, while statistically significant, represent modest clinical changes. The practical significance depends on baseline obesity severity, intervention context, and whether improvements are sustained long-term. Some studies showed no significant anthropometric changes despite increased physical activity, possibly reflecting compensatory dietary behaviors or insufficient activity increases to create meaningful energy deficits.
Participant characteristics influenced outcomes. Some evidence suggests stronger effects in participants with existing overweight or obesity compared to normal-weight youth [6]. This finding has clinical relevance, as it suggests wearables may be particularly valuable as treatment tools rather than solely for prevention in healthy-weight populations. The summary of evidence for effectiveness of wearable devices in pediatric obesity management is discussed in Figure 2 [6, 29].
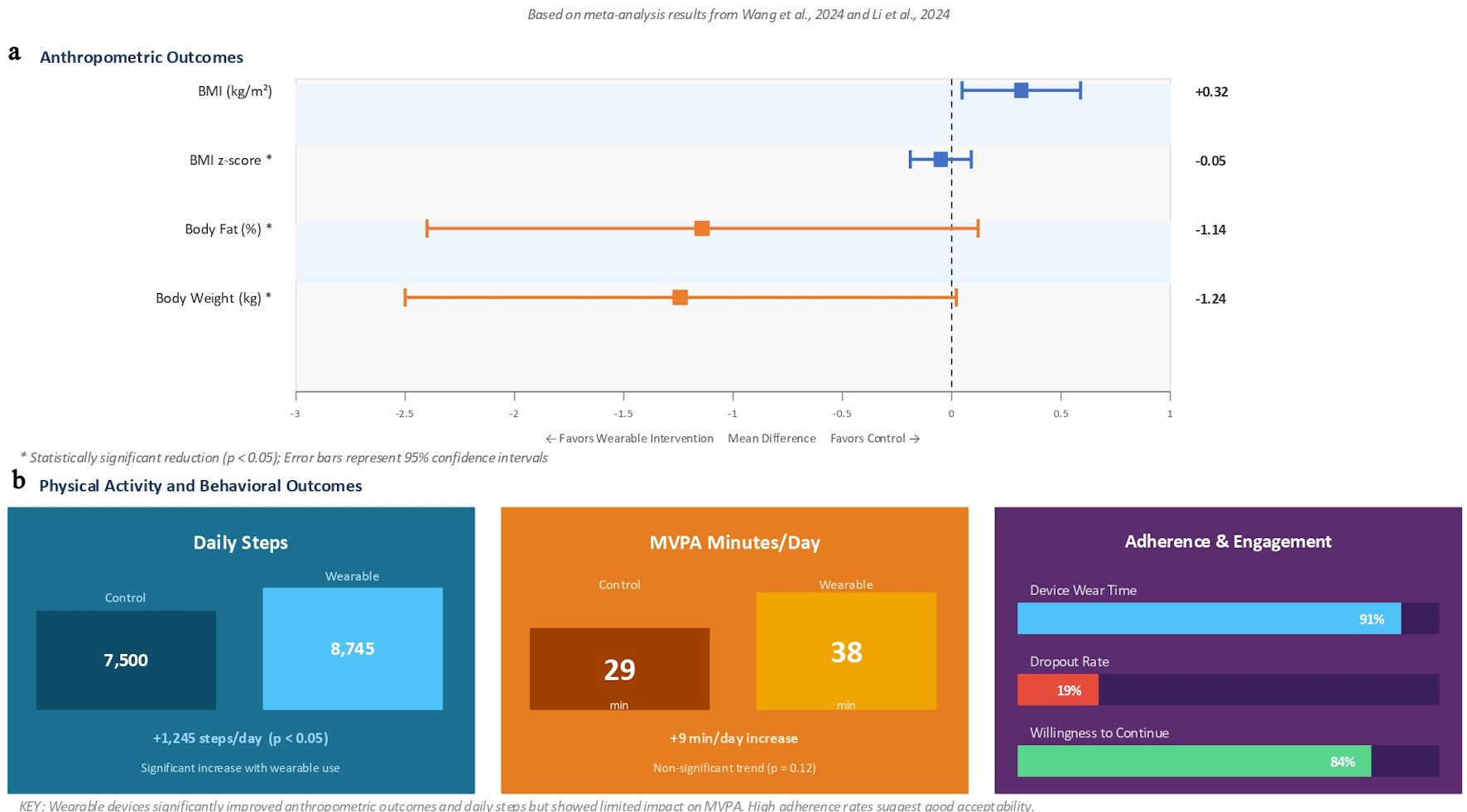 Click for large image | Figure 2. Summary of effective evidence for wearable devices in pediatric obesity. This figure summarizes meta-analysis results demonstrating the effectiveness of wearable device interventions across multiple outcome domains. (a) Anthropometric outcomes showing mean differences favoring wearable device interventions compared to controls. BMI decreased by 0.50 kg/m2 (95% CI, –0.90 to –0.11; P = 0.01), BMI z-score decreased by 0.05 (95% CI, –0.09 to –0.01; P = 0.03), body fat percentage decreased by 1.14% (95% CI, –2.17% to –0.11%, P = 0.03), and body weight decreased by 1.26 kg (95% CI, –2.32 to –0.20 kg; P = 0.02). All outcomes showed statistically significant improvements (P < 0.05) with error bars representing 95% CIs. (b) Physical activity and behavioral outcomes. Daily step count increased significantly by 1,205 steps per day (95% CI, 626 to 1,784 steps; P < 0.001) comparing wearable device users to controls, demonstrating robust effects on ambulatory physical activity. However, MVPA minutes per day showed only a non-significant increase of 3 min (P = 0.08), indicating that more research is needed to understand impacts on MVPA specifically. Adherence and engagement metrics demonstrated favorable patterns: device wear time averaged 91% of days, dropout rate was 19%, and 85% of participants reported willingness to continue using devices after study completion, suggesting high acceptability and feasibility in pediatric populations (based on meta-analysis results from Wang et al, 2022 [6] and Au et al, 2024 [29]). BMI: body mass index; CI: confidence interval; MVPA: moderate-to-vigorous physical activity. |
Behavioral and psychosocial outcomes
Beyond physical and anthropometric outcomes, wearable devices may influence health behaviors and psychological factors. Studies have examined changes in dietary behaviors, screen time, sleep patterns, motivation, and self-efficacy [30].
A digital health program combining Fitbit trackers with text-based health coaching for adolescents with obesity showed significant improvements in tracked daily active minutes (P = 0.006) and steps (P < 0.001) over 12 weeks [31]. Notably, 85% of participants reported wanting to continue wearing the Fitbit after the study ended, and adherence was high with devices worn on 91.1% of days on average.
Preliminary evidence suggests CGM use may enhance dietary awareness and facilitate behavior change. In feasibility studies, youth with obesity reported that seeing real-time glucose responses to food intake helped them understand the metabolic impact of their choices [19]. This represents a novel mechanism by which wearables could support obesity management beyond simply tracking activity.
Sleep monitoring capabilities of modern wearables offer another potential benefit. Poor sleep quality and insufficient sleep duration are recognized risk factors for pediatric obesity [32]. Devices that track sleep patterns and provide feedback may help families identify and address sleep problems, though research specifically examining sleep interventions via wearables in pediatric obesity remains limited.
| Feasibility and Acceptability in Pediatric Populations | ▴Top |
Device adherence and wear time
Adherence to wearing devices represents a critical factor determining intervention success. Studies report variable wear time depending on device type, participant age, study duration, and intervention components. In the meta-analysis by Wang et al, dropout rates across studies ranged from 3.9% to 52.0%, with an average of 19.3% [6].
Research examining accelerometer use in obesity treatment found that over 90% of children provided at least 4 days of valid accelerometer data, though only about half provided complete 7-day data [33]. Parental interviews revealed challenges including discomfort from elastic belts, concerns about social stigma (particularly at school), and device loss or breakage.
Consumer-grade devices often show better long-term adherence than research-grade accelerometers, likely due to more appealing designs, lighter weight, and features like display screens showing real-time feedback. A study of adolescents with obesity using Fitbits documented 91% wear time over 12 weeks, substantially higher than typical research accelerometer adherence [31].
Age-related considerations
Age significantly influences both device preference and effective use. Younger children (under 10 years) show less understanding of device purpose and may lack motivation to independently engage with the data [34]. Parental involvement becomes crucial in these age groups. Studies show that when parents also use wearables, child motivation and adherence improve markedly.
Adolescents generally demonstrate higher autonomous motivation for device use compared to younger children. However, adolescents aged 10 to 12 years may show peak motivation, with interest potentially declining in older teens [34]. This suggests developmentally tailored approaches are needed across the pediatric age spectrum.
Device aesthetics and social acceptability matter considerably. Children express preferences for wrist-worn over waist-worn devices due to convenience and style [35]. Color options, customizable faces, and branded designs (Disney, Marvel characters) enhance appeal to younger users. Adolescents may prefer devices that look like regular watches rather than obviously medical or research equipment.
Safety and tolerability
Safety data from studies using wearable devices in pediatric obesity populations has been reassuring. Reported adverse events are minimal and primarily consist of minor skin irritation at sensor sites [17, 36]. No serious device-related adverse events have been documented in published literature.
CGM devices in youth with obesity demonstrate safety profiles similar to those observed in populations with diabetes. Skin reactions occur in a small percentage of users but typically resolve after device removal [20, 21]. The noninvasive nature of most activity tracking devices (accelerometers, pedometers) poses minimal risk beyond potential loss or breakage.
One consideration specific to obesity populations relates to device fit and comfort. Some wearables may not accommodate larger body sizes, particularly arm-worn devices. Manufacturers have begun addressing this by offering adjustable and extended bands, but clinicians should verify appropriate fit when recommending devices.
| Clinical Applications and Integration Into Care | ▴Top |
Use as assessment tools
Wearable devices serve valuable roles as objective assessment instruments in pediatric obesity clinics. Baseline physical activity assessment using accelerometry provides quantitative data to inform treatment planning and goal setting. This represents an improvement over subjective recall methods that often overestimate activity levels [37].
Monitoring during treatment allows clinicians to track progress objectively and identify patients who may need additional support or intervention modification. Real-world activity patterns captured by wearables reveal information not obtainable through clinic-based fitness testing alone [38].
Research applications have benefited substantially from wearable technology. Studies examining environmental interventions, school-based programs, and community initiatives use objective activity measurement to evaluate effectiveness. This has strengthened the evidence base for various obesity prevention strategies [39].
Use as intervention tools
Beyond assessment, wearables function as active intervention components through several mechanisms. Self-monitoring represents a core behavioral change technique. The simple act of wearing a device and viewing one’s data increases awareness and may prompt behavior change [40].
Goal-setting features enable users to work toward personalized targets. Many devices allow customization of step goals, active minutes, or other metrics appropriate to individual capabilities and progression. Achieving goals triggers visual or haptic feedback that provides immediate positive reinforcement.
Gamification elements enhance engagement, particularly for younger users. Virtual rewards, badges, animated characters, and competitive challenges tap into motivational systems relevant to children and adolescents [41]. Some devices enable family or peer challenges that leverage social motivation.
Integration with smartphone applications expands functionality. Apps provide detailed data visualization, trend analysis, and educational content. Some support coaching features where counselors can view patient data remotely and provide feedback or encouragement between visits [31].
Challenges in clinical implementation
Despite potential benefits, several barriers impede widespread clinical adoption of wearables in pediatric obesity management. Cost represents a significant consideration, as devices range from $30 for basic pedometers to over $300 for advanced smartwatches. Insurance coverage for obesity-related wearables remains limited, creating access disparities.
Data management poses technical challenges. Clinicians need systems to receive, store, analyze, and act on data from patient devices. Electronic health record integration remains underdeveloped for wearable data. Without streamlined workflows, reviewing individual patient activity data becomes impractical in busy clinical settings.
Privacy and data security concerns require attention, particularly for pediatric populations. Policies must address data ownership, parental access, sharing permissions, and protection against unauthorized use. Compliance with regulations like HIPAA (Health Insurance Portability and Accountability Act) and COPPA (Children’s Online Privacy Protection Act) adds complexity to implementation [42].
Staff training and time represent additional considerations. Clinicians need education on device capabilities, data interpretation, and how to incorporate wearable information into counseling. Developing these competencies requires investment in professional development. Summary of key RCTs and systematic reviews on wearable devices in the management of pediatric obesity are discussed in Table 1 [6, 19–21, 29–31, 33, 34, 36].
 Click to view | Table 1. Summary of Key Randomized Controlled Trials and Systematic Reviews on Wearable Devices in Pediatric Obesity |
| Limitations and Knowledge Gaps | ▴Top |
Methodological limitations
Current evidence faces several methodological limitations. Study heterogeneity in terms of device types, intervention components, duration, and outcome measures limits ability to draw definitive conclusions. Standardization of protocols would strengthen future research.
Many studies lack long-term follow-up data. Evaluations typically span weeks to months, leaving questions about sustained effectiveness and behavior change maintenance. Weight regain following initial loss represents a major challenge in obesity treatment, yet few wearable device studies report outcomes beyond the active intervention period [43].
Control group selection presents challenges. Some studies compare wearables to no intervention, while others use wearables plus behavioral counseling versus counseling alone. These different comparison approaches yield different effect size estimates and make synthesis across studies difficult.
Publication bias may inflate apparent effectiveness. Studies showing positive results are more likely to be published than those with null findings. The relatively small number of studies in some device categories limits robust assessment of publication bias through methods like funnel plots.
Device-related limitations
Accuracy issues persist for certain activities and populations. Most devices perform best for ambulatory activities like walking or running but show reduced accuracy for activities involving upper body movement, cycling, or water sports [44]. This potentially underestimates total activity in children who engage heavily in these activities.
Validity in younger children requires further study. Most validation research has focused on school-age children and adolescents. Preschool-aged children present unique challenges due to sporadic, intermittent movement patterns [13].
Battery life and maintenance requirements affect real-world adherence. Devices requiring daily charging may experience lower wear rates than those with week-long battery life. Durability concerns also arise, as children may subject devices to rougher treatment than adult users.
Algorithm limitations affect energy expenditure estimation. Predicted calorie expenditure from wearables shows substantial variation and may not be sufficiently accurate for precise energy balance calculations [45]. Height, weight, and body composition influence accuracy, potentially affecting performance in obese populations.
Implementation and sustainability gaps
Evidence for integration into clinical care pathways remains limited. Most studies represent researcher-initiated interventions rather than clinic-initiated programs. Models for sustainable implementation in real-world healthcare settings require development and testing.
Optimal intervention “dose” remains unclear. Questions persist regarding ideal device features, intervention duration, intensity of additional support (coaching, feedback, incentives), and timing of interventions across development. Precision medicine approaches may ultimately reveal that optimal strategies vary by individual characteristics.
Cost-effectiveness data are largely absent. Decision-makers need information on the costs of device provision, data management infrastructure, and personnel time relative to health benefits achieved. Current evidence cannot definitively answer whether wearable-based interventions represent good value compared to alternative approaches.
Health equity implications deserve attention. If effective, wearables could exacerbate disparities if access remains concentrated among higher-income families. Alternatively, the declining cost of basic activity trackers might make them more equitable than some interventions. Research specifically examining effectiveness across socioeconomic groups would inform equitable implementation. Additionally, significant gaps exist regarding racial and ethnic disparities in wearable device effectiveness. Most studies included in existing systematic reviews were conducted in high-income countries, predominantly the United States, United Kingdom, Australia, and Northern Europe [6, 29, 38], with limited representation of low- and middle-income countries and underserved populations. Consequently, it remains unclear whether findings are generalizable across diverse racial, ethnic, and socioeconomic groups. Geographic variation in access to wearable technologies is also underexplored; children in rural and low-resource settings face distinct barriers including limited internet connectivity for data syncing, fewer retail options for device purchase, and reduced access to healthcare providers who can integrate device data into clinical care. Few included studies reported subgroup analyses by race, ethnicity, or socioeconomic status, limiting the ability to assess whether observed effects are generalizable across diverse populations. Advantages, limitations and clinical considerations for different types of wearable devices in pediatric obesity, along with cost ranges and age specific recommendations are outlined in Tables 2 and 3 [35–45].
Click to view | Table 2. Advantages, Limitations, and Clinical Considerations for Different Types of Wearable Devices in Pediatric Obesity |
Click to view | Table 3. Age-Specific Recommendations |
| Future Directions and Recommendations | ▴Top |
Research priorities
Several research priorities emerge from current evidence gaps. Large-scale, long-term RCTs with standardized outcome measures would strengthen the evidence base. These should include diverse populations to ensure generalizability and examine potential effect modifiers like age, sex, obesity severity, and socioeconomic status.
Comparative effectiveness research could identify optimal device types and features for different subgroups. Head-to-head comparisons of pedometers versus sophisticated multi-sensor devices, or consumer-grade versus research-grade accelerometers, would guide cost-effective selection.
Intervention component studies using factorial designs could disentangle effects of device provision alone versus devices combined with goal setting, feedback, incentives, or counseling. Understanding active ingredients would enable more efficient interventions.
Mechanistic research examining pathways by which wearables influence behavior would inform intervention enhancement. Do effects primarily result from increased awareness, goal-setting structures, immediate feedback, or other mechanisms? Different mechanisms might suggest different optimal uses.
Implementation science investigations should examine strategies for successful integration into clinical practice and community programs. Hybrid effectiveness-implementation trials could simultaneously evaluate clinical outcomes and implementation processes.
Technology development needs
Device manufacturers should prioritize several improvements. Enhanced accuracy across diverse activities and populations, particularly for children at different developmental stages, would increase utility. Algorithms specifically developed and validated for pediatric populations would improve precision.
Extended battery life and improved durability would enhance real-world adherence. Water-resistant or waterproof designs enable wear during all activities. Hypoallergenic materials and adjustable sizing accommodate diverse users, including those with larger body sizes.
Sophisticated data analytics and artificial intelligence could provide more meaningful insights than simple activity summaries. Pattern recognition algorithms might identify barriers to activity or opportunities for intervention personalization. Predictive models could alert clinicians to patients at risk for disengagement.
Privacy-preserving designs that give families control over data while enabling clinical use represent important priorities. Secure data transmission, transparent privacy policies, and child-appropriate consent processes would address current concerns.
Clinical and policy recommendations
Clinicians considering wearable devices for pediatric obesity management should view them as potentially useful adjuncts rather than standalone solutions. Devices work best when embedded within comprehensive behavioral interventions including nutrition counseling, behavior modification strategies, and family engagement.
Selection of appropriate devices should consider patient age, preferences, family resources, and intervention goals. For basic activity promotion, simple pedometers may suffice and minimize cost barriers. More sophisticated needs might warrant advanced multi-sensor devices.
Goal setting should be individualized and progressive. Starting with achievable targets based on baseline data and gradually increasing expectations can promote sustained engagement and self-efficacy. Goals should focus on behaviors (e.g., active minutes, step counts) rather than purely on weight outcomes, to maintain motivation even if weight loss plateaus.
Family involvement enhances effectiveness, particularly for younger children. Encouraging parents to also use wearables and participate in activity challenges creates shared experiences and parental modeling of healthy behaviors.
Policy makers should consider expanding insurance coverage for wearable devices as part of intensive behavioral therapy for pediatric obesity. Evidence supporting effectiveness in increasing physical activity justifies inclusion among covered services. Coverage policies should specify appropriate clinical contexts and follow-up requirements.
School-based implementations offer potential for population-level impact. Policies supporting school physical activity programs that incorporate wearable technology could reach large numbers of children, including those from families unable to afford devices independently.
Research funding priorities should emphasize pragmatic trials in real-world settings, studies in underserved populations, and investigations of sustained effectiveness and cost-effectiveness. Comparative effectiveness research would guide evidence-based device selection and implementation strategies.
| Conclusions | ▴Top |
Wearable devices have emerged as promising tools in the comprehensive management of pediatric obesity. Current evidence demonstrates that activity trackers, accelerometers, and related technologies can increase physical activity levels and improve anthropometric outcomes in children and adolescents with obesity. Devices are generally feasible and acceptable to pediatric populations when thoughtfully selected and implemented. Emerging applications including CGM and integrated smartwatch platforms expand the potential scope of wearable technology beyond traditional activity tracking.
However, significant knowledge gaps and implementation challenges temper enthusiasm. Effect sizes for anthropometric outcomes remain modest. Long-term sustainability of behavior changes and weight loss remains uncertain. Heterogeneity in study designs and intervention components limits definitive conclusions about optimal approaches. Cost, data management, privacy concerns, and equity considerations pose barriers to widespread clinical adoption.
The rapid evolution of wearable technology, including multi-sensor integration and artificial intelligence capabilities, offers expanding possibilities but also poses challenges, as studied devices may become obsolete before definitive evidence accumulates. Advancing this field will require sustained collaboration among researchers, clinicians, technology developers, policy makers, and families to build the evidence base, ensure devices meet clinical needs, and implement findings in practice. Ultimately, wearable devices represent tools, not solutions in themselves. Their effectiveness depends on how they are integrated into comprehensive, family-centered, behaviorally grounded obesity treatment approaches. When used appropriately within supportive contexts, wearables offer objective monitoring, real-time feedback, and engagement-enhancing features that may strengthen traditional interventions. As the pediatric obesity epidemic continues to demand innovative responses, wearable technology stands as one promising avenue worthy of continued investigation, thoughtful implementation, and careful evaluation.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare no conflicts of interest related to this manuscript.
Author Contributions
VSC was responsible for conceptualization, literature review, manuscript drafting, and critical revision. VG contributed to the conceptualization, literature review, manuscript drafting, and critical revision. JRP contributed to the conceptualization, literature review, manuscript drafting, and critical revision. SG contributed to the literature review, manuscript drafting, and critical revision. All authors approved the final manuscript.
Data Availability
This review article is based exclusively on published literature. No original data was generated. All cited references are accessible through their respective publishers. The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
BMI: body mass index; CGM: continuous glucose monitor; CI: confidence interval; COPPA: Children’s Online Privacy Protection Act; GPS: global positioning system; HIPAA: Health Insurance Portability and Accountability Act; HR: heart rate; MVPA: moderate-to-vigorous physical activity; PPG: photoplethysmography; RCT: randomized controlled trial; ROC–AUC: receiver operating characteristic–area under the curve; TAR: time above range; TIR: time in range
| References | ▴Top |
- Global Atlas on Childhood Obesity [Internet]. World Obesity Federation. Available from: https://www.worldobesity.org/membersarea/global-atlas-on-childhood-obesity.
- Freedman DS, Mei Z, Srinivasan SR, Berenson GS, Dietz WH. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: the Bogalusa Heart Study. J Pediatr. 2007;150(1):12-17.e12.
doi pubmed - Lobstein T, Jackson-Leach R, Moodie ML, Hall KD, Gortmaker SL, Swinburn BA, James WP, et al. Child and adolescent obesity: part of a bigger picture. Lancet. 2015;385(9986):2510-2520.
doi pubmed - Gurnani M, Birken C, Hamilton J. Childhood obesity: causes, consequences, and management. Pediatr Clin North Am. 2015;62(4):821-840.
doi pubmed - Ho M, Garnett SP, Baur L, Burrows T, Stewart L, Neve M, Collins C. Effectiveness of lifestyle interventions in child obesity: systematic review with meta-analysis. Pediatrics. 2012;130(6):e1647-1671.
doi pubmed - Wang W, Cheng J, Song W, Shen Y. The effectiveness of wearable devices as physical activity interventions for preventing and treating obesity in children and adolescents: systematic review and meta-analysis. JMIR Mhealth Uhealth. 2022;10(4):e32435.
doi pubmed - Prensky M. Digital natives, digital immigrants. On the Horizon. 2001;9(5):1-6.
- Brickwood KJ, Watson G, O'Brien J, Williams AD. Consumer-based wearable activity trackers increase physical activity participation: systematic review and meta-analysis. JMIR Mhealth Uhealth. 2019;7(4):e11819.
doi pubmed - Direito A, Carraca E, Rawstorn J, Whittaker R, Maddison R. mHealth technologies to influence physical activity and sedentary behaviors: behavior change techniques, systematic review and meta-analysis of randomized controlled trials. Ann Behav Med. 2017;51(2):226-239.
doi pubmed - Welk GJ, Corbin CB, Dale D. Measurement issues in the assessment of physical activity in children. Res Q Exerc Sport. 2000;71(2 Suppl):S59-73.
pubmed - Trost SG, McIver KL, Pate RR. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sports Exerc. 2005;37(11 Suppl):S531-543.
doi pubmed - Chandler JL, Brazendale K, Beets MW, Mealing BA. Classification of physical activity intensities using a wrist-worn accelerometer in 8-12-year-old children. Pediatr Obes. 2016;11(2):120-127.
doi pubmed - Byun W, Lee JM, Kim Y, Brusseau TA. Classification accuracy of a wearable activity tracker for assessing sedentary behavior and physical activity in 3-5-year-old children. Int J Environ Res Public Health. 2018;15(4).
doi pubmed - Hazell TJ, Ellery CV, Cohen TR, Vanstone CA, Rodd CJ, Weiler HA. Assessment of pedometer accuracy in capturing habitual types of physical activities in overweight and obese children. Pediatr Res. 2016;80(5):686-692.
doi pubmed - Rowlands AV, Eston RG. Comparison of accelerometer and pedometer measures of physical activity in boys and girls, ages 8-10 years. Res Q Exerc Sport. 2005;76(3):251-257.
doi pubmed - Klonoff DC, Ahn D, Drincic A. Continuous glucose monitoring: a review of the technology and clinical use. Diabetes Res Clin Pract. 2017;133:178-192.
doi pubmed - Hegedus E, Salvy SJ, Wee CP, Naguib M, Raymond JK, Fox DS, Vidmar AP. Use of continuous glucose monitoring in obesity research: a scoping review. Obes Res Clin Pract. 2021;15(5):431-438.
doi pubmed - Li C, Ford ES, Zhao G, Mokdad AH. Prevalence of pre-diabetes and its association with clustering of cardiometabolic risk factors and hyperinsulinemia among U.S. adolescents: National Health and Nutrition Examination Survey 2005-2006. Diabetes Care. 2009;32(2):342-347.
doi pubmed - Chimatapu SN, Mittelman SD, Klomhaus A, Vu MH, Habib M, Wisk LE, Black DS, et al. The effect of continuous glucose monitoring feedback on glycaemic variability in youth with obesity: A within-participant feasibility study. Pediatr Obes. 2025;20(10):e70035.
doi pubmed - Vidmar AP, Naguib M, Raymond JK, Salvy SJ, Hegedus E, Wee CP, Goran MI. Time-limited eating and continuous glucose monitoring in adolescents with obesity: a pilot study. Nutrients. 2021;13(11):3697.
doi pubmed - Simunovic M, Kumric M, Rusic D, Paradzik Simunovic M, Bozic J. Continuous glucose monitoring-new diagnostic tool in complex pathophysiological disorder of glucose metabolism in children and adolescents with obesity. Diagnostics (Basel). 2024;14(24):2801.
doi pubmed - Danne T, Nimri R, Battelino T, Bergenstal RM, Close KL, DeVries JH, Garg S, et al. International consensus on use of continuous glucose monitoring. Diabetes Care. 2017;40(12):1631-1640.
doi pubmed - Gillinov S, Etiwy M, Wang R, Blackburn G, Phelan D, Gillinov AM, Houghtaling P, et al. Variable accuracy of wearable heart rate monitors during aerobic exercise. Med Sci Sports Exerc. 2017;49(8):1697-1703.
doi pubmed - Henriksen A, Haugen Mikalsen M, Woldaregay AZ, Muzny M, Hartvigsen G, Hopstock LA, Grimsgaard S. Using fitness trackers and smartwatches to measure physical activity in research: analysis of consumer wrist-worn wearables. J Med Internet Res. 2018;20(3):e110.
doi pubmed - Perez SA, Diaz AM, Lopez DM. Personalized tracking of physical activity in children using a wearable heart rate monitor. Int J Environ Res Public Health. 2020;17(16).
doi pubmed - Brage S, Wedderkopp N, Franks PW, Andersen LB, Froberg K. Reexamination of validity and reliability of the CSA monitor in walking and running. Med Sci Sports Exerc. 2003;35(8):1447-1454.
doi pubmed - Liden CB, Wolowicz M, Stivoric J, Teller A, Vishnubhatla S, Farringdon J. Accuracy and reliability of the SenseWear™ armband as an energy expenditure assessment device. 2002.
- Zhou Q, Wang D, Mhurchu CN, Gurrin C, Zhou J, Cheng Y, Wang H. The use of wearable cameras in assessing children's dietary intake and behaviours in China. Appetite. 2019;139:1-7.
doi pubmed - Au WW, Recchia F, Fong DY, Wong SHS, Chan DKC, Capio CM, Yu CCW, et al. Effect of wearable activity trackers on physical activity in children and adolescents: a systematic review and meta-analysis. Lancet Digit Health. 2024;6(9):e625-e639.
doi pubmed - Goran Dankovic, Tomislav Stantic, Romina Herodek, Stevan Stamenkovic, Nenad Stojiljkovic, Boban Jelenkovic, et al. Effects of commercially available wearable devices on physical activity promotion and health in children and adolescents: systematic review. Applied sciences. 2023;13(12):7194.
- Cummings C, Crochiere R, Lansing AH, Patel R, Stanger C. A digital health program targeting physical activity among adolescents with overweight or obesity: open trial. JMIR Pediatr Parent. 2022;5(1):e32420.
doi pubmed - Hart CN, Cairns A, Jelalian E. Sleep and obesity in children and adolescents. Pediatr Clin North Am. 2011;58(3):715-733.
doi pubmed - Robertson W, Stewart-Brown S, Wilcock E, Oldfield M, Thorogood M. Utility of accelerometers to measure physical activity in children attending an obesity treatment intervention. J Obes. 2011;2011:398918.
doi pubmed - Ridgers ND, McNarry MA, Mackintosh KA. Feasibility and effectiveness of using wearable activity trackers in youth: a systematic review. JMIR Mhealth Uhealth. 2016;4(4):e129.
doi pubmed - Schaefer SE, Van Loan M, German JB. A feasibility study of wearable activity monitors for pre-adolescent school-age children. Prev Chronic Dis. 2014;11:E85.
doi pubmed - Kalantar HT, Kalantar AT, Alali M, Alali N, Naji H. Effectiveness of telehealth and wearable device-based interventions for managing childhood and adolescent obesity: a systematic review and meta-analysis. Cureus. 2025;17(10):e94551.
doi pubmed - Corder K, Ekelund U, Steele RM, Wareham NJ, Brage S. Assessment of physical activity in youth. J Appl Physiol (1985). 2008;105(3):977-987.
doi pubmed - Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EM, Andersen LB, et al. Objectively measured physical activity and sedentary time in youth: the International children's accelerometry database (ICAD). Int J Behav Nutr Phys Act. 2015;12:113.
doi pubmed - Janssen X, Mann KD, Basterfield L, Parkinson KN, Pearce MS, Reilly JK, Adamson AJ, et al. Development of sedentary behavior across childhood and adolescence: longitudinal analysis of the Gateshead Millennium Study. Int J Behav Nutr Phys Act. 2016;13:88.
doi pubmed - Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28(6):690-701.
doi pubmed - Cugelman B. Gamification: what it is and why it matters to digital health behavior change developers. JMIR Serious Games. 2013;1(1):e3.
doi pubmed - Huckvale K, Torous J, Larsen ME. Assessment of the data sharing and privacy practices of smartphone apps for depression and smoking cessation. JAMA Netw Open. 2019;2(4):e192542.
doi pubmed - Hall KD, Kahan S. Maintenance of lost weight and long-term management of obesity. Med Clin North Am. 2018;102(1):183-197.
doi pubmed - Hills AP, Mokhtar N, Byrne NM. Assessment of physical activity and energy expenditure: an overview of objective measures. Front Nutr. 2014;1:5.
doi pubmed - Evenson KR, Goto MM, Furberg RD. Systematic review of the validity and reliability of consumer-wearable activity trackers. Int J Behav Nutr Phys Act. 2015;12:159.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
International Journal of Clinical Pediatrics is published by Elmer Press Inc.