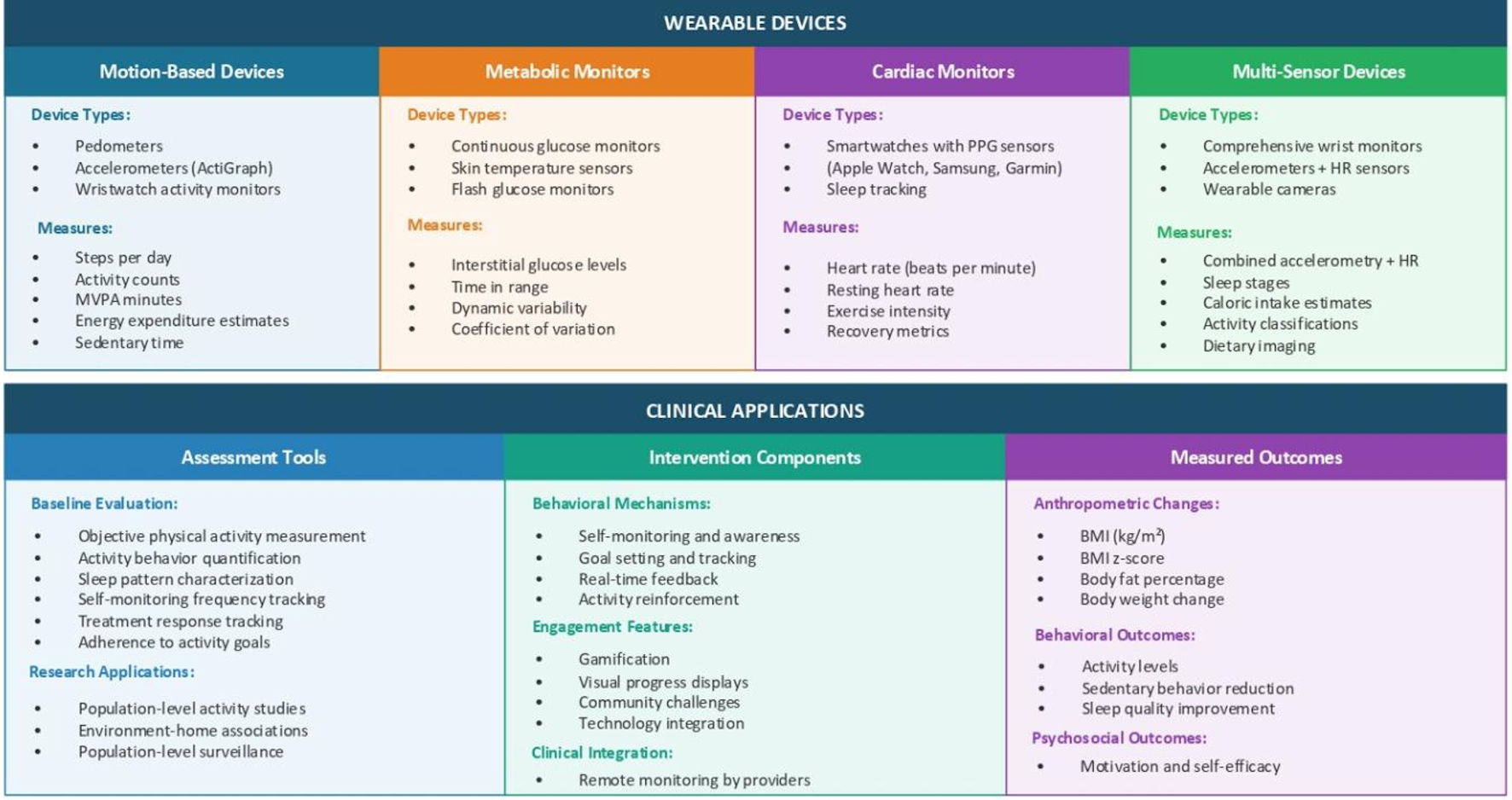
↓ Figure 1. Classification and clinical applications of wearable devices in pediatric obesity management. This figure illustrates the four main categories of wearable devices used in pediatric obesity research and clinical practice. The top panel shows device classification: 1) motion-based devices including pedometers, accelerometers (ActiGraph), consumer trackers (Fitbit, Garmin), and wristband activity monitors, which measure steps per day, distance traveled, active minutes, MVPA duration, energy expenditure estimate, and sedentary time; 2) metabolic monitors including continuous glucose monitors (FreeStyle Libre, Dexcom), real-time CGM (RT-CGM), and flash glucose monitoring, which measure interstitial glucose levels, TIR, time above/below range, glycemic variability, glucose excursions, and coefficient of variation; 3) cardiac monitors including smartwatches with PPG sensors (Apple Watch, Samsung Galaxy), Polar HR monitors, and chest strap monitors, which measure HR (beats per minute), HR variability, resting HR, exercise intensity zones, cardio fitness score, and recovery metrics; 4) multi-sensor devices including SenseWear armband, ActiHeart, wearable cameras, and smart clothing/textiles, which combine accelerometry with HR, heat flux, galvanic skin response, skin temperature, sleep stages, and dietary imaging. The lower panel depicts clinical applications across three domains: 1) assessment tools (baseline evaluation including objective physical activity measurement, sedentary behavior quantification, and sleep pattern characterization; ongoing monitoring including treatment response tracking, adherence to activity goals, and real-world behavior patterns; research applications including intervention effectiveness studies, environmental factor associations, and population-level surveillance); 2) intervention components (behavioral mechanisms including self-monitoring and awareness, goal-setting and tracking, real-time feedback, and positive reinforcement; engagement features including gamification elements, social connectivity/challenges, visual progress displays, and achievement rewards; clinical integration including remote monitoring by providers); and 3) measured outcomes (anthropometric changes including BMI, BMI z-score, body fat percentage, body weight, and waist circumference; behavioral outcomes including physical activity levels, sedentary behavior reduction, and dietary awareness/modification; psychosocial outcomes including motivation and self-efficacy). MVPA: moderate-to-vigorous physical activity; PPG: photoplethysmography; TIR: time in range; HR: heart rate; BMI: body mass index.