| International Journal of Clinical Pediatrics, ISSN 1927-1255 print, 1927-1263 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Int J Clin Pediatr and Elmer Press Inc |
| Journal website https://ijcp.elmerpub.com |
Original Article
Volume 15, Number 2, June 2026, pages 62-68

Efficacy and Safety of Ketamine Infusions in Pediatric Patients With Acute Pain Related to Sickle Cell Disease
Sarah Shelleya, Sandra Tayb, Catherine Rothb, Kanda Strohlb, Joseph D. Tobiasb, c, d, Giorgio Venezianob, c, Grant Heydingerb, c
aHeritage College of Osteopathic Medicine - Dublin, Ohio and Ohio University, Athens, OH, USA
bDepartment of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital and the Department of Anesthesiology & Pain Medicine, Columbus, OH, USA
cDepartment of Anesthesiology & Pain Medicine, The Ohio State University College of Medicine, Columbus, OH, USA
dCorresponding Author: Joseph D. Tobias, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH 43205, USA
Manuscript submitted March 26, 2026, accepted April 24, 2026, published online May 22, 2026
Short title: Ketamine and Sickle Cell Disease
doi: https://doi.org/10.14740/ijcp1057
| Abstract | ▴Top |
Background: When pain associated with sickle cell disease (SCD) escalates, adjunctive agents including ketamine are increasingly employed as part of multimodal pain management strategies. Ketamine enhances analgesic effects when used in conjunction with opioids, often allowing for reduced opioid requirements and mitigating associated adverse effects such as tolerance, dependence, and respiratory depression. In the adult population, subanesthetic ketamine infusions have been used in non-critical care settings as an adjunct to opioid analgesia.
Methods: We retrospectively reviewed our experience with the use of a ketamine infusion outside of the pediatric intensive care unit setting for complex pain uncontrolled by opioids related to SCD in pediatric-aged patients. The study cohort included patients ≤ 21 years of age who received continuous ketamine infusions for SCD-related pain over a 10-year period at a tertiary pediatric hospital.
Results: The study cohort included 51 patients and 141 hospitalizations, with ketamine initiated at a mean starting rate of 0.10 ± 0.03 mg/kg/h and administered for a median duration of 4 days. Adverse events occurred in 24 out of the 51 patients in the cohort during at least one hospitalization, resulting in infusion discontinuation in 12 patients. Hallucinations and dizziness were the most frequently reported events. Infusion discontinuation due to lack of efficacy occurred in seven patients.
Conclusions: Our findings demonstrate that, with standardized protocols, staff education, and appropriate monitoring, ketamine infusions can be safely administered outside of the intensive care unit for pediatric patients with SCD experiencing severe pain.
Keywords: Ketamine; Pain management; Sickle cell vaso-occlusive crisis
| Introduction | ▴Top |
Sickle cell disease (SCD) is a multisystem, autosomal recessive disorder caused by a mutation in the β-globin gene, which leads to the production of an abnormal form of hemoglobin known as hemoglobin S (HbS). HbS has a different molecular structure than normal adult hemoglobin, causing erythrocytes to be rigid, with increased adhesion properties, and sickle-shaped, impairing laminar flow through micro-vessels [1]. SCD occurs more commonly in individuals of African, Mediterranean, Middle Eastern, Indian, and Caribbean descent, but can be found in people of any ethnicity [2]. The term “sickle cell disease” is broadly used to encompass a wide range of sickle hemoglobinopathies that vary in severity and clinical presentation while the abovementioned mutation in the β hemoglobin chain is the most common form of the disease when individuals are homozygous for the HbS allele [1].
The hallmark symptom of SCD is recurrent episodes of severe pain, sudden in onset, throbbing and sharp, known as vaso-occlusive crises (VOCs) [1]. VOCs result from the obstruction of small blood vessels by sickled erythrocytes and multicellular aggregates, which include adherent white blood cells, platelets, and other elements [2, 3]. These clusters disrupt laminar flow and the microcirculation, leading to tissue ischemia followed by reperfusion injury when normal flow resumes. This sequence of events triggers oxidative and inflammatory stress, producing severe pain typically in the lower back, limbs, and joints. VOCs may be preceded by a prodromal phase and tend to peak within a few days before resolving. These crises can also lead to serious complications such as acute chest syndrome, stroke, and multi-organ damage [3]. Vaso-occlusive events are the most frequent cause of hospital admissions among patients with SCD and significantly disrupt daily life, including school and work attendance [4].
The primary approach to managing pain caused by SCD involves prompt initiation of individualized opioid analgesia, with dosing guided by prior patient history, when available, to optimize efficacy. Common opioids used include morphine and hydromorphone, administered via oral, intravenous, or other routes depending on the clinical context, with frequent reassessment to adjust dosing as needed [3]. Adjuvant therapies such as acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) are routinely used alongside opioids to enhance pain control and reduce opioid requirements, which is critical given the risk of opioid tolerance and hyperalgesia [3, 5].
When pain associated with SCD escalates, adjunctive agents including ketamine are increasingly employed as part of multimodal pain management strategies. Ketamine enhances analgesic effects when used in conjunction with opioids, often allowing for reduced opioid requirements and mitigating associated adverse effects such as tolerance and respiratory depression [6]. Evidence from observational and retrospective studies supports ketamine’s opioid-sparing potential and clinical utility in both acute and chronic pain settings, including pediatric patients with VOCs [6–8]. Notably, subanesthetic ketamine infusions have been used effectively in non-critical care settings to reduce pain scores and opioid use in pediatric patients experiencing sickle cell crises [7]. Additionally, ketamine reduces daily opioid demand, even among patients with multiple admissions for SCD-related pain, independent of prior opioid exposure or co-analgesic therapy [8]. We present preliminary experience with the use of a ketamine infusion outside of the pediatric intensive care unit (PICU) setting for complex pain uncontrolled by opioids related to sickle cell VOC. We discuss our multidisciplinary pathway developed for ketamine infusions outside of the ICU setting, including patient monitoring, investigate our initial clinical experience, and review its adverse effect and safety profile in pediatric patients with pain related to SCD.
| Materials and Methods | ▴Top |
This retrospective cohort study was approved by the Institutional Review Board of Nationwide Children’s Hospital (STUDY00001488) in accordance with the principles stated in the Declaration of Helsinki. As a retrospective study using de-identified data, the need for individual written informed consent was waived. The study cohort included patients ≤ 21 years of age who received a ketamine infusion for the treatment of pain caused by SCD over a 10-year period (January 2015 through February 28, 2025). Patients were identified through the records of the Acute Pain Service, the Pharmacy Database, and the EPIC Data Warehouse.
For each patient, demographic data were collected including age, weight, height, gender, race/ethnicity, and comorbid conditions. Ketamine specific data included the starting infusion rate, average daily infusion rate, and any rate adjustments. The duration of therapy, adverse effects related to the ketamine infusion including, but not limited to delirium, hallucinations, agitation, salivation, nausea, and vomiting, and information regarding why the ketamine infusion was stopped or rate adjustment were noted. Adjunctive agents used to specifically treat adverse effects with ketamine including benzodiazepines, anti-emetics, and glycopyrrolate (anti-sialagogue) were recorded.
Ketamine protocol
A standardized ketamine policy and protocol was created for the hospital prior to the use of ketamine infusions outside of the ICU setting. The protocol outlined the use of ketamine infusions on the inpatient hematology/oncology ward as an adjunct to pain management for acute pain unrelieved by opioid infusion. This policy, its introduction to our institution, and initial experience with the use of ketamine to treat pain in pediatric oncology patients with high-risk neuroblastoma undergoing chemotherapy with dinutuximab have been previously reported [9].
To allow for the administration of ketamine outside of the ICU setting, this hospital protocol and policy was used to guide patient selection, dosing, monitoring, and nursing care. Inpatient nursing staff completed mandatory education prior to caring for these patients through the hospital online learning system. This education provided information about the use of ketamine for analgesia, dosing, adverse effects, patient monitoring, and documentation requirements in the electronic medical record (EMR). After completion of the module, the nurses completed a post-course test to document competency and receive credit for completion. Information about the use of ketamine for analgesia was also added to the hospital’s pain management intranet website. Ketamine infusions for analgesia including dosing and other care were managed by consultation with either the Acute Pain Service or the Palliative Care Service [9].
Ketamine infusions were used as part of a multimodal regimen for severe pain that was non-responsive or under-responsive to common agents and techniques for analgesia, including opioids delivered by patient-controlled analgesia (PCA). An order set reflecting the institutional policy was added to the EMR. The recommended starting dose for a continuous IV ketamine infusion was 0.025–0.1 mg/kg/h with dose escalation up to a maximum of 0.4 mg/kg/h. Patients receiving ketamine were monitored with continuous pulse oximetry during the infusion. Additional monitoring included blood pressure, heart rate, and respiratory rate, as well as pain scores and level of consciousness. These were assessed by the nursing staff every 30 min for the first hour, then hourly for the next 2 h, followed by every 4 h for the remainder of the infusion. Symptoms of adverse central nervous system effects (excessive sedation, altered mental status) were assessed every 30 min for the first hour, and then hourly for the duration of the infusion. The level of pain was monitored based on the patient’s age and level of cognition using a self-report scale or an observational scale every 4 h (Table 1).
 Click to view | Table 1. Ketamine Policy and Protocol for Ketamine Infusions Outside of the ICU Setting |
Statistical analysis
All data were summarized using standard descriptive statistics. Categorical variables were presented as frequencies and percentages, and continuous variables were summarized as mean and standard deviation or median and interquartile range (IQR), as appropriate. To assess whether the occurrence of adverse events was associated with daily ketamine infusion rate or total infusion duration, we used linear mixed-effects models with a random intercept for patient ID to account for within-patient correlation among individuals with multiple hospitalizations. A two-sided P-value < 0.05 was considered statistically significant. Analyses were performed using R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
| Results | ▴Top |
The study cohort included 51 patients. The demographic data of the study cohort are listed in Table 2. As several patients had multiple hospital admissions over the study period, we included data for up to five hospital admissions from an individual patient, resulting in a total of 141 hospitalizations (Fig. 1). The median number of hospitalizations per patient was 2 (IQR, 1–5 hospitalizations). The median age at first admission was 17 years (IQR, 14–19 years) and 51% of patients were female. All patients identified as non-Hispanic Black. The median hospital length of stay was 10 days (IQR, 7–14 days). Ketamine infusions were initiated at a mean starting dose of 0.10 ± 0.03 mg/kg/h and administered for a median duration of 4 days (IQR, 2–7 days). When considering the 141 hospitalizations in these 51 patients, ketamine was infused for a total of 709 days.
Click to view | Table 2. Demographic Characteristics of the Study Population |
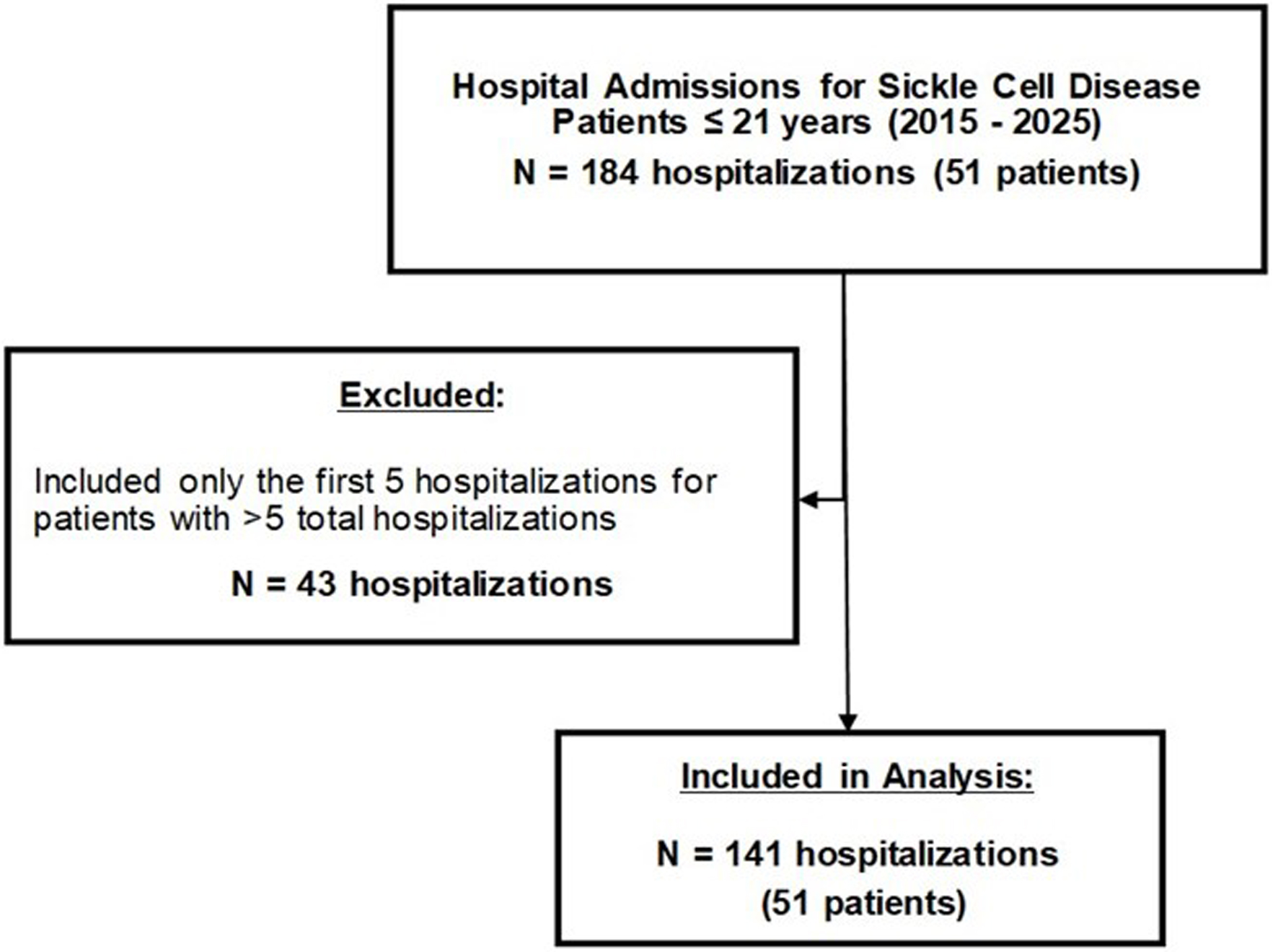 Click for large image | Figure 1. Flow diagram of patient identification and inclusion of hospitalizations in the retrospective cohort evaluating ketamine infusions for sickle cell disease-related pain. |
When evaluating adverse events at the patient level, 24 out of the 51 patients (47.1%) in the cohort experienced at least one adverse event during one hospitalization, resulting in infusion discontinuation in 12 patients. At the hospitalization level, adverse events occurred in 33 out of 141 hospitalizations (23.4%), leading to infusion discontinuation in 18 cases. Infusion discontinuation due to lack of efficacy occurred in seven patients and eight hospitalizations (Table 2).
The most commonly reported adverse events were hallucinations and dizziness, each occurring in 10 hospitalizations and affecting nine and 10 patients, respectively. Other reported adverse events included delirium (five hospitalizations), nausea (four hospitalizations), agitation, sedation, pruritus, and blurry vision (three hospitalizations each). Some hospitalizations included multiple adverse events (Table 3). The occurrence of adverse events was not significantly associated with either average daily ketamine infusion rate or total infusion duration. Patients with an adverse event had an estimated 0.004 mg/kg/h higher infusion rate (P = 0.33) and an estimated 1.28-day shorter infusion duration (P = 0.11) compared to those without an adverse event (Fig. 2). All of the adverse effects were recognized and treated without the need to escalate care (PICU transfer) or call the Rapid Response Team.
Click to view | Table 3. Adverse Events by Hospitalization and Patient |
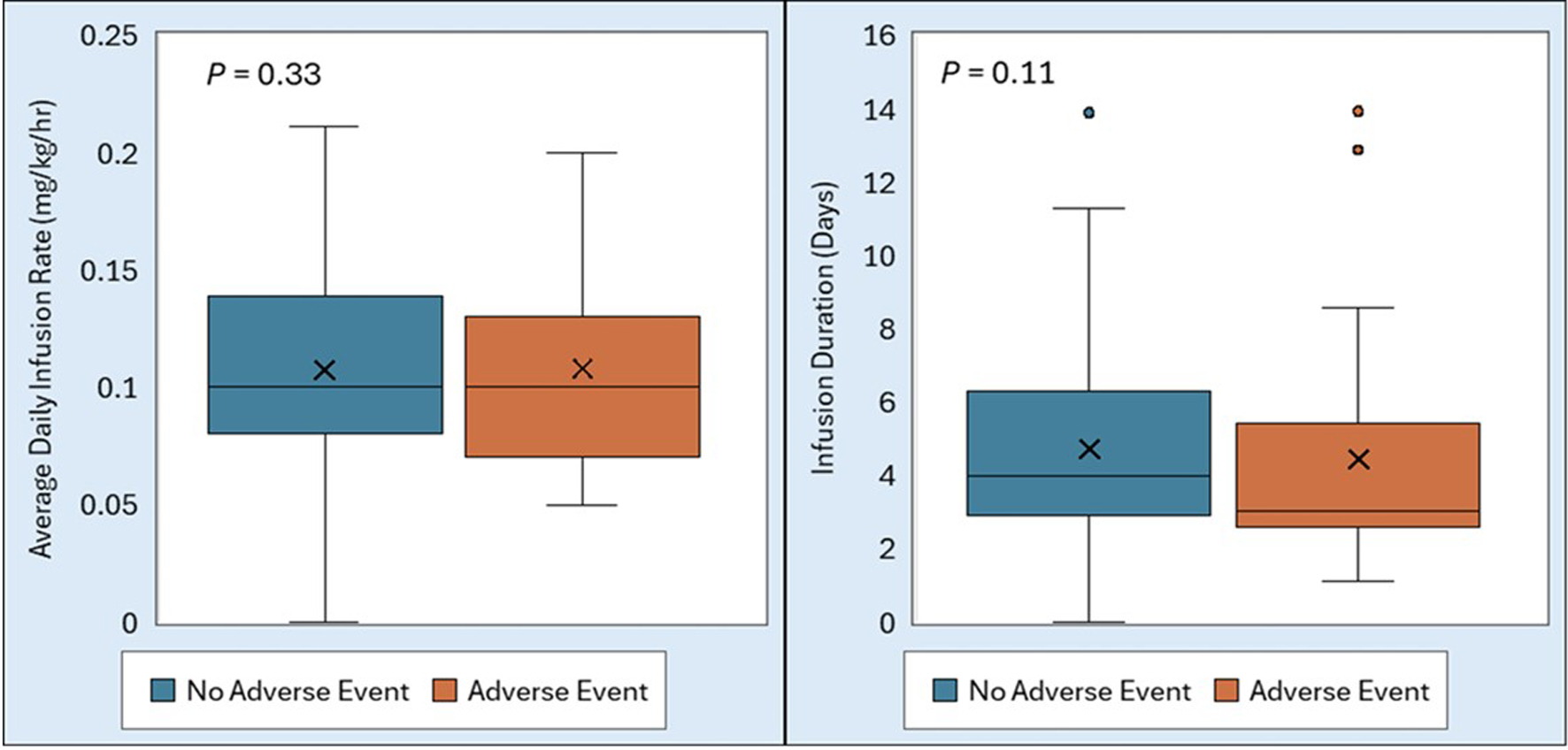 Click for large image | Figure 2. Distribution of ketamine infusion rate (left) and infusion duration (right) by occurrence of adverse events. P-values from linear mixed-effects models indicate no significant association. |
| Discussion | ▴Top |
Ketamine at subanesthetic doses has been increasingly used in pediatric pain management protocols as a targeted adjunct for postoperative pain, complex pain syndromes, including VOCs in SCD and neuropathic pain related to oncologic therapy [10]. Its use spans a range of inpatient contexts and has extended beyond critical care settings as demonstrated by our study cohort, with structured protocols enabling safe administration on general pediatric inpatient wards. The current study outlines our initial clinical experience over 10 years with a novel pathway to allow for ketamine infusions to treat pain in sickle cell patients outside of the ICU setting. In our cohort of 51 pediatric patients and 141 hospitalizations, ketamine infusions were administered using a standardized institutional protocol and were generally well tolerated. Adverse events occurred in 23.4% of hospitalizations and resulted in infusion discontinuation in 12.8% of cases. Importantly, the occurrence of adverse events was not significantly associated with either the average daily ketamine infusion rate or the duration of therapy. Adverse effects were recognized and treated without care escalation. These findings add to the clinical experience with an emphasis on pediatric-aged patients, demonstrating that subanesthetic ketamine infusions can be administered safely on non-ICU pediatric units with appropriate monitoring and institutional protocols.
Outside of the perioperative setting, previous studies have suggested that ketamine infusions may help control pain and reduce cumulative opioid exposure during hospitalizations for VOCs [10–14]. The first of these published in 2010 was a small case series evaluating low-dose ketamine for acute vaso-occlusive pain in five pediatric patients, who received ketamine either as an adjunct to opioid PCA (n = 4) or as monotherapy (n = 1) [11]. Ketamine was administered by bolus dosing and continuous infusion, with infusion rates ranging from 0.2 to 0.6 mg/kg/h. Following initiation of the ketamine infusion, apparent benefit was noted in three of the five patients with two having significantly improved pain control with a low-dose ketamine infusion, whereas one additional patient had a significant reduction in opiate utilization. Adverse effects were reported in two patients and included nystagmus, hypertension, unresponsiveness in the setting of a possible inadvertent bolus, and dysphoria; however, no adverse effects were observed in the remaining patients.
In a retrospective cross-sectional study of 46 admissions in 22 patients with SCD (mean age of 15 years), a subanesthetic ketamine infusion decreased pain scores within 24 h of the start of the initiation in 34 of 46 admissions [12]. In the remaining 12 admissions, there was a decrease in pain scores after ≥ 24 h of ketamine initiation. Additionally, there was a decrease in the average oral morphine equivalents of 122.8 mg/day after the initiation of the ketamine infusion. Similar to our study, the starting ketamine infusion rate ranged from 0.02 to 0.15 mg/kg/h (0.09 ± 0.03 mg/kg/h) with a maximum infusion rate range of 0.03 to 0.21 mg/kg/h (0.11 ± 0.04 mg/kg/h). The infusions were administered from 4.4 to 109 h (52.7 ± 25.30 h). Adverse effects occurred in 11 (23.9%) admissions with only four requiring cessation of the infusion. However, the introduction of ketamine into the pain management regimens did not reduce the number of admissions when comparing the year following ketamine initiation relative to the year prior.
In a randomized, prospective, double-blind, non-inferiority trial of 240 pediatric patients (7 to 18 years of age) with severe VOC pain (pain score ≥ 7 of 10), the pain regimen was randomized to either a bolus dose of ketamine (1 mg/kg) or morphine (0.1 mg/kg) administered intravenously [13]. Pain was assessed using a Numerical Rating Scale (NRS) pain score. Baseline NRS pain scores (8.9 vs. 9.2) were similar between the two groups. Ketamine demonstrated non-inferiority to morphine when comparing the maximum change in NRS pain scores (66.4% vs. 61.3%). The average time to achieve maximum reduction in NRS pain scores was shorter with ketamine than morphine (19.8 versus 34.1 min) although the average duration of analgesia was less with ketamine. Patients who received ketamine were 11.3 times more likely to develop adverse effects (37.5% versus 3.3%), although these were transient and non-life-threatening. The authors concluded that intravenous ketamine (1 mg/kg) provides comparable analgesic effectiveness as intravenous morphine in the treatment of acute, severe pain related to sickle cell crisis, although it is associated with a higher incidence of transient, non-life-threatening adverse effects. They further noted that it can be a reliable alternative to morphine in the management of severe painful sickle cell crisis, especially in a resource-limited environment.
More recently, a large retrospective case series summarized a single-center’s experience with the use of ketamine for the inpatient management of pain related to SCD during 156 admissions in adolescents and young adults over a 6-year period [14]. The median starting dose of ketamine was 2 µg/kg/min with a median maximum dose of 3 µg/kg/min. The ketamine was started a median of 13.7 h after admission and infused for a median of 3 days. In the majority of encounters, the ketamine infusion was discontinued prior to discontinuation of the opioid PCA. Efficacy was demonstrated by a reduction in opioid requirements in 79.3% of the encounters. Adverse effects were noted in 34 of the encounters (21.8%). The most common adverse effects were mild and nonlife-threatening, including dizziness (5.6%), hallucinations (5.1%), dissociation (2.6%), and sedation (1.9%).
The same group of authors have also provided a more extensive systemic review published in 2021, which summarizes clinical experience from 18 published works from January 2010 through December 2019 [15]. The majority of reported experiences outlined dosing from 0.1 to 0.3 mg/kg/h, concluding that ketamine is a safe and effective treatment for pain related to VOC from SCD and that it should be considered more widely. The authors cautioned that the significant variability among published clinical studies regarding dosing, timing of initiation, duration of infusion, and timing of discontinuation highlights the need for standardized ketamine infusion protocols for the management of these patients.
Using the currently described infusion protocol, we have previously demonstrated the successful and safe use of ketamine as an adjunct to dinutuximab-induced neuropathic pain in pediatric oncology patients, with infusions improving patient comfort while limiting the need for escalating opioid doses [9]. In that cohort, as in our current study, ketamine was generally well tolerated without safety concerns. Across both populations, reported adverse effects most commonly included hallucinations, dysphoria, dizziness, and hypersalivation. These effects were typically transient and responsive to supportive measures such as benzodiazepines or anticholinergic medications. In our current study, hallucinations and dizziness were the most frequently reported adverse events, but the overall rate of infusion discontinuation remained low. These findings reinforce the concept that ketamine-related adverse effects are dose-related, manageable, and rarely require termination of therapy when patients are appropriately monitored. An important observation from our analysis was the lack of association between adverse event occurrence and either ketamine infusion rate or infusion duration. This suggests that within the dosing range used in our institutional protocol (0.025–0.4 mg/kg/h), titration of ketamine to achieve analgesia does not appear to significantly increase the likelihood of adverse events. This finding supports the safety of individualized dose adjustments when managing severe pain that is refractory to conventional opioid therapy.
Beyond its safety profile, the use of ketamine as part of a multimodal analgesic strategy has important clinical implications for patients with SCD. Recurrent VOCs frequently lead to repeated hospitalizations and prolonged opioid exposure, increasing the risk of opioid tolerance, hyperalgesia, and dependence. By providing NMDA receptor antagonism and modulating central sensitization pathways, ketamine offers a mechanism to enhance analgesia while potentially reducing opioid requirements. The ability to administer ketamine infusions safely outside the ICU also has important implications for hospital resource utilization by avoiding unnecessary ICU admissions for patients who otherwise require ward-level care.
Several limitations should be considered when interpreting the findings of this study. The retrospective design and lack of a control group limit the ability to establish causal relationships and may introduce selection bias. We decided to limit chart review to five hospital admissions per patient in an attempt to avoid over-representing any one patient with multiple admissions and yet result in a sample size that allowed successful completion of the chart reviews while obtaining an adequate study size to ensure that the data were accurate. This study was conducted at a single tertiary pediatric institution with an established ketamine protocol and specialized acute pain and palliative care services, which may limit generalizability to centers without similar infrastructure. Given the issue studied, the age of the patients was at the higher end of the pediatric age group (range of our study cohort was 14–19 years) and as such, applicability to younger patients may not be feasible. Additionally, documentation of pain scores and analgesic response was variable in the medical record, limiting our ability to quantify the analgesic efficacy and opioid-sparing effects. Future prospective studies are needed to better characterize the impact of ketamine infusions on pain control, opioid consumption, and patient-reported outcomes in pediatric patients with SCD.
Despite these limitations, this study adds to the growing literature supporting the safe use of ketamine infusions for complex pain syndromes in pediatric populations. Our findings demonstrate that with standardized protocols, staff education, and appropriate monitoring, ketamine infusions can be safely administered outside of the ICU for children with SCD experiencing severe pain. The final caveat is that this is report from a single-center, with a highly trained nursing staff and specialized pain/palliative care services. As such, one may not be able to generalize our findings and experience to hospitals without such an infrastructure.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
As a retrospective review, the need for individual informed consent was waived by the IRB review.
Author Contributions
SS: chart review, preparation of initial and subsequent drafts including finial version; KS, GV, GH: pathway development, patient care, review of final draft; ST: data analysis and manuscript preparation including review of final draft; CR: data collection, data analysis and manuscript preparation including review of final draft; JDT: project leader, review of drafts including final manuscript.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
| References | ▴Top |
- Elendu C, Amaechi DC, Alakwe-Ojimba CE, Elendu TC, Elendu RC, Ayabazu CP, Aina TO, et al. Understanding Sickle cell disease: Causes, symptoms, and treatment options. Medicine (Baltimore). 2023;102(38):e35237.
doi pubmed - Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. 2010;376(9757):2018-2031.
doi pubmed - Darbari DS, Sheehan VA, Ballas SK. The vaso-occlusive pain crisis in sickle cell disease: Definition, pathophysiology, and management. Eur J Haematol. 2020;105(3):237-246.
doi pubmed - Bou-Maroun LM, Meta F, Hanba CJ, Campbell AD, Yanik GA. An analysis of inpatient pediatric sickle cell disease: Incidence, costs, and outcomes. Pediatr Blood Cancer. 2018;65(1):e26758.
doi pubmed - Brandow AM, Carroll CP, Creary S, Edwards-Elliott R, Glassberg J, Hurley RW, Kutlar A, et al. American Society of Hematology 2020 guidelines for sickle cell disease: management of acute and chronic pain. Blood Adv. 2020;4(12):2656-2701.
doi pubmed - Vadivelu N, Schermer E, Kodumudi V, Belani K, Urman RD, Kaye AD. Role of ketamine for analgesia in adults and children. J Anaesthesiol Clin Pharmacol. 2016;32(3):298-306.
doi pubmed - Masaracchia MM, Sites BD, Lee J, Thomas JJ, Fernandez PG. Subanesthetic ketamine infusions for the management of pediatric pain in non-critical care settings: An observational analysis. Acta Anaesthesiol Scand. 2019;63(9):1225-1230.
doi pubmed - Zavala NA, Knoebel RW, Anitescu M. Lidocaine and ketamine infusions as adjunctive pain management therapy: a retrospective analysis of clinical outcomes in hospitalized patients admitted for pain related to sickle cell disease. Front Pain Res (Lausanne). 2022;3:878985.
doi pubmed - Streby KA, Tobias JD, McPhaden E, Downie S, Stanek J, Roth C, Patel PO. Ketamine infusion as an adjunct to opioid analgesia in pediatric patients with high-risk neuroblastoma undergoing treatment with Dinutuximab: adverse effects and safety in a non-ICU setting. J Pain Res. 2025;18:283-292.
doi pubmed - Neri CM, Pestieau SR, Darbari DS. Low-dose ketamine as a potential adjuvant therapy for painful vaso-occlusive crises in sickle cell disease. Paediatr Anaesth. 2013;23(8):684-689.
doi pubmed - Zempsky WT, Loiselle KA, Corsi JM, Hagstrom JN. Use of low-dose ketamine infusion for pediatric patients with sickle cell disease-related pain: a case series. Clin J Pain. 2010;26(2):163-167.
doi pubmed - Onyebuchi CO, Chumpitazi CE, Placencia JL, Jackson AN, Jones JL, Torres L, Tubman VN. Ketamine for pain in sickle cell disease reduces opioid usage. J Pain Symptom Manage. 2024;67(3):e169-e175.
doi pubmed - Lubega FA, DeSilva MS, Munube D, Nkwine R, Tumukunde J, Agaba PK, Nabukenya MT, et al. Low dose ketamine versus morphine for acute severe vaso occlusive pain in children: a randomized controlled trial. Scand J Pain. 2018;18(1):19-27.
doi pubmed - Harris EM, Vilk E, Donado C, Williams A, Heeney MM, Solodiuk J, Greco C, et al. Ketamine use for management of vaso-occlusive pain in pediatric sickle cell disease. Pediatr Blood Cancer. 2023;70(5):e30254.
doi pubmed - Harris EM, Vilk E, Heeney MM, Solodiuk J, Greco C, Archer NM. A systematic review of ketamine for the management of vaso-occlusive pain in sickle cell disease. Pediatr Blood Cancer. 2021;68(7):e28989.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
International Journal of Clinical Pediatrics is published by Elmer Press Inc.