| International Journal of Clinical Pediatrics, ISSN 1927-1255 print, 1927-1263 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Int J Clin Pediatr and Elmer Press Inc |
| Journal website https://ijcp.elmerpub.com |
Case Report
Volume 15, Number 2, June 2026, pages 69-73

A Case of Peanut Aspiration: Double Whammy
Fleur Kabalaa, Craig Schrammb, c, Nancy Groverd, e
aUniversity of Connecticut School of Medicine, Farmington, CT 06030-6322, USA
bPediatric Sleep Center, Connecticut Children’s Medical Center, Hartford, CT 06106-3322, USA
cDepartment of Pediatrics, University of Connecticut School of Medicine, Farmington, CT 06030-6322, USA
dDepartment of Pediatric Otolaryngology Head and Neck Surgery, Connecticut Children’s, Hartford, CT 06106-3322, USA
eCorresponding Author: Nancy Grover, Department of Pediatric Otolaryngology Head and Neck Surgery, Connecticut Children’s, Hartford, CT 06106-3322, USA
Manuscript submitted December 18, 2025, accepted March 24, 2026, published online May 22, 2026
Short title: A Case of Peanut Aspiration
doi: https://doi.org/10.14740/ijcp1038
| Abstract | ▴Top |
Pediatric foreign body aspiration remains a significant health hazard with potentially severe complications and fatal outcomes. We present case of a 14-month-old child who developed two severe complications: post obstructive pulmonary edema and acute respiratory distress syndrome with a very protracted 59-day hospital course after choking on a peanut. It required a multidisciplinary approach and use of cryoprobe to remove the foreign body which was challenging due to its location and severe respiratory instability. Although both these complications have been individually described after foreign body aspiration, this is the first case report of these in same patient. This case highlights the decision-making algorithm and use of an uncommon approach to remove peanut in a worst case scenario. It emphasizes the need for continued outreach to improve awareness of choking hazards in pediatric population.
Keywords: Foreign body; Peanut; Aspiration; Complications; Pulmonary edema; Respiratory distress syndrome; Cryotherapy
| Introduction | ▴Top |
Tracheobronchial foreign body (FB) is one of the most common acute and severe diseases in children. Symptoms vary depending on the size, grade of obstruction, and the location of the FB. These can cause several complications, including potentially fatal complications—post obstructive pulmonary edema (POPE) and acute respiratory distress syndrome (ARDS) [1–9]. Use of cryoprobe for removal of pediatric airway FBs has been reported; however, it is not common practice [10–15]. Its application in a critical patient with an FB in a challenging location is novel. This case reports a 14-month-old who developed both POPE and ARDS following an obstruction of the left mainstem bronchus after aspirating a peanut, leading to several medical and surgical complications leading to a 59-day hospital course.
| Case Report | ▴Top |
A previously healthy 14-month-old male presented to an outside emergency department (ED) after aspirating a peanut. Chest X-ray at an outside hospital revealed complete whiteout of the left lung, suggestive of an FB obstruction of the left bronchus. He was transferred to Connecticut Children’s (CCMC) via Emergency Medical Services, arriving with oxygen saturations in the 80s while receiving 15 L/min of oxygen via facemask.
On arrival, he was in visible respiratory distress with a respiratory rate of 41 breaths/min and oxygen saturations of 75% on high flow. A repeat chest X-ray showed complete collapse of the left lung, now with leftward mediastinal shift. The child was rushed to the operating room (OR) for bronchoscopy and peanut fragment removal where he quickly desaturated to 55–65% and became obtunded.
He was intubated with rapid sequence induction. On rigid bronchoscopy a large fragment of peanut was visualized in the left mainstem bronchus. Multiple attempts at retrieval were made with optical grasping resulting in more fragmented remnants; significant mucosal inflammation and friability further made it challenging. Severe left lung bleeding occurred after extracting a large fragment, likely from release of obstruction and underlying parenchymal hemorrhage. The patient was intubated into the right mainstem bronchus to avoid blood spillover into the right lung; bleeding was controlled with oxymetazoline. A fragment became embedded in the left lingular segmental bronchus. With worsening respiratory status, a pediatric pulmonologist was consulted. Remnant oozing was stopped with epinephrine, and flexible bronchoscopic removal with Dormia basket was attempted, but unsuccessful. Given the frequent, sustained desaturations and airway inflammation, it was deemed safer to abandon the procedure.
The patient remained intubated and was returned to the pediatric intensive care unit (PICU) for ongoing airway management, including high-dose intravenous steroids and antibiotics. His respiratory status remained fragile over next day.
A chest computed tomography (CT) scan performed revealed the previously visualized peanut fragment near the takeoff to the lingula and findings suggestive of bilateral POPE (Figs. 1 and 2).
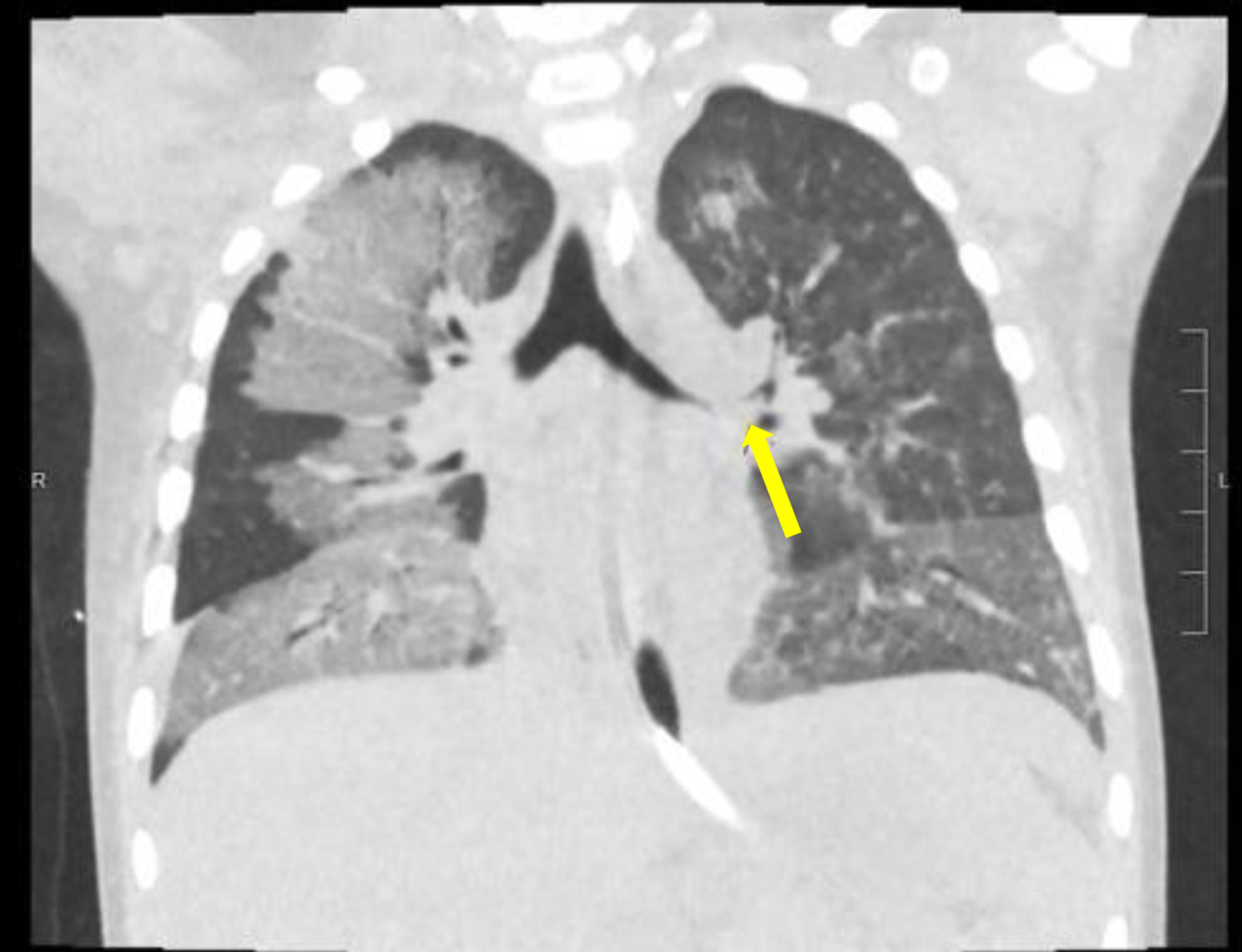 Click for large image | Figure 1. Non-contrast coronal computed tomography (CT) scan of chest showing the peanut fragment (yellow arrow) in left upper lobe bronchus located at the junction of the takeoff of the lingular and left upper lobe bronchus. |
 Click for large image | Figure 2. Non-contrast axial computed tomography (CT) scan of chest showing ground-glass opacification with a perihilar and anteroposterior dependent distribution. |
However, he failed to respond to medical management for POPE over the next 48 h, with escalating ventilation needs concerning for ARDS. With failure to respond to intensive medical management, concerns arose about the remnant peanut fragment causing airway inflammation. His respiratory status remained tenuous, worsening over 48 h. Ventilator settings remained with a high positive end-expiratory pressure (PEEP) of 12, fraction of inspired oxygen (FiO2) fluctuating up to 100%, and oxygen saturation dropping to 70s. Hence after intense multidisciplinary discussion involving otolaryngology, pulmonary and critical care teams and anesthesiologists, it was believed that the small segment of peanut was likely contributing to continued respiratory compromise, due to inflammation and partial obstruction of the lung. Hence a decision was made to return to OR for removal of the peanut despite his fragile respiratory status. Requirement for high PEEP precluded the use of a rigid bronchoscope, hence decision for a flexible bronchoscopy through the existing endotracheal tube. At that time factors prompting use of cryoprobe were fragment location in segmental bronchus and airway inflammation. Cryotherapy-assisted removal was performed using a flexible bronchoscope, which dislodged multiple fragments from the left segmental bronchus into the trachea and was followed by a retrieval basket. The patient was transferred back to the PICU. However, his respiratory status did not improve. Airway cultures were negative at that time. He required several ventilatory support measures including high-frequency oscillatory ventilation (HFOV), with consideration for extracorporeal membrane oxygenation (ECMO). He developed recurrent right pneumothorax, both times treated successfully with chest tubes. He was extubated on day 43 after multiple failed attempts complicated by prolonged intubation, steroids, muscle relaxants, and atelectasis causing deconditioning. He underwent rehabilitation on the floor and was discharged from hospital day 59 on room air.
| Discussion | ▴Top |
FB aspiration is the primary cause of accidental death in children under the age of 1 [16] with a peak between 19 and 24 months [17]. Trends in choking-related deaths have remained steady over past several years [18], highlighting the need for continued vigilance, outreach, and education. Most frequently aspirated FBs are organic materials (67%) like peanuts [19] with the right mainstem bronchus being the most common site of impaction (38%) [20]. Typical presenting symptoms are respiratory distress, coughing, and wheezing.
Our patient presented with acute dyspnea from sudden airway obstruction. His X-ray demonstrated complete left lung atelectasis, which along with escalating oxygen requirements, portended severe respiratory compromise and ultimately led to the development of POPE and ARDS.
His initial CT scan demonstrated central, nondependent ground glass opacification, findings characteristic of POPE, or negative pressure pulmonary edema (NPPE) [21]. POPE has two subclasses: type 1, characterized by forced inspiration against an obstructed airway, and type 2 occurring after relief of chronic obstruction. Most reported pediatric cases follow acute upper airway obstruction from croup, epiglottitis, or FB aspiration [3–5]. Ringold et al reported two cases of POPE after life-threatening episode of choking on food, both these and other cases had a fairly swift recovery within 24–36 h without sequelae.
Although one case of POPE from lower tracheal obstruction has been reported [1], none from bronchial obstruction have been described. In our case, it is possible that the peanut initially lodged in his glottis, contributing to classic negative pressure and POPE. Additionally, given children’s compliant chest walls, even main bronchial obstruction, may have been sufficient to generate significant negative pressure needed to cause POPE.
The events triggering ARDS in our patient remain somewhat conjectural but likely involve alveolar-capillary barrier disruption, impaired fluid clearance, and oxidative/mechanical injury. These processes may be incited by infectious and direct or systemic and indirect insults [22, 23]. Mechanical ventilation can worsen ARDS through volutrauma and barotrauma to healthy lung regions. Shear stress in healthy regions from repetitive opening and closing of alveoli through the breathing cycle also contributes [24]. Re-expansion pulmonary edema (RPE), though more common after evacuation of a pneumothorax or pleural effusion, has also occurred even with re-expansion of a briefly collapsed lung [25, 26], as may have been in our case. This is similarly caused by alveolar capillary injury. Hemorrhagic pulmonary edema progressing to ARDS has also been associated with RPE [27].
Severe respiratory distress in children due to FB aspiration has been documented, typically involving delayed or missed diagnosis, causing progressive inflammation. One notable case involved a 2-year-old child, misdiagnosed with asthma, later found to have bilateral peanut aspiration [8]. Others included a 6-year-old who aspirated cement and an 11-year-old who aspirated a pushpin, both developing ARDS and all cases required ECMO [9, 28]. Our patient’s airway cultures were negative, but it is possible that the proinflammatory properties demonstrated by peanut oil [29] may have contributed to the lung injury, especially if some smaller fragments remained in distal airways. Arachidonic acid release from retained organic FBs can cause local inflammation, mucus plugging, atelectasis, and pneumonia [30]. Hazards of peanut aspiration have been appreciated for over a century. A 1919 publication on “Arachidic bronchitis” described several children who presented with severe respiratory symptoms and toxic sickness from aspirated peanut ranging from 1 to 48 days [31]. Again, rapid deterioration, such as in our patient, with short exposure history has not been borne out in this century.
Given the patient’s deterioration, we felt it essential to remove the retained peanut fragment. Requirements for high PEEP and its location in an acutely angled segmental bronchus made rigid bronchoscopy unfeasible, so we engaged our pulmonary colleagues for flexible bronchoscopic removal. Previous attempts using a Dormia basket had failed, and to minimize airway trauma and excessive manipulation, we employed cryoprobe removal which makes direct contact with FBs and is most suited for organic FBs which have a high-water content. While more commonly used in adults, it has had limited use in children [10–13] with most being case series [32]. Recent publications have quoted overall success rates ranging from 91.7% to 94% for FB removal [15]. However, adjunct techniques are often required (30%) [15], as in ours where the dislodged fragment was retrieved with Dormia basket.
FB aspiration continues to remain a significant hazard for the younger pediatric population. With advanced bronchoscopic techniques and critical care at a tertiary pediatric hospital, although we were able to achieve a good outcome in this child, continued public awareness and education to prevent this situation in the first place will achieve the best outcome.
Acknowledgments
The authors would like to acknowledge the patient and their family for their contribution to this educational case.
Financial Disclosure
This work received no specific funding.
Conflict of Interest
The authors report no conflict of interest.
Informed Consent
Patient consent was obtained in accordance with ethical standards.
Author Contributions
Craig Schramm contributed to validation, and manuscript review/editing; Nancy Grover led conceptualization and supervision in addition to validation, and review/editing; and Fleur Serena Kabala contributed to drafting and review/editing of the manuscript. All authors contributed to the conception and design of the report, data acquisition, manuscript drafting, and critical revision for important intellectual content; all authors approved the final manuscript and agree to be accountable for all aspects of the work.
Data Availability
The authors declare that data supporting the findings of this study are available within the article, and additional information is available from the corresponding author upon reasonable request.
| References | ▴Top |
- Bashir A, Ahmad SQ, Silverman J, Concepcion E, Lee H. Post-obstructive pulmonary edema from aspirated nuts. SAGE Open Med Case Rep. 2017;5:2050313X17717391.
doi pubmed - Ringold S, Klein EJ, Del Beccaro MA. Postobstructive pulmonary edema in children. Pediatr Emerg Care. 2004;20(6):391-395.
doi pubmed - Capitanio MA, Kirkpatrick JA. Obstructions of the upper airway in children as reflected on the chest radiograph. Radiology. 1973;107(1):159-161.
doi pubmed - Travis KW, Todres ID, Shannon DC. Pulmonary edema associated with croup and epiglottitis. Pediatrics. 1977;59(5):695-698.
pubmed - Soliman MG, Richer P. Epiglottitis and pulmonary oedema in children. Can Anaesth Soc J. 1978;25(4):270-275.
doi pubmed - Brown KL, Shefler A, Cohen G, DeMunter C, Pigott N, Goldman AP. Near-fatal grape aspiration with complicating acute lung injury successfully treated with extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2003;4(2):243-245.
doi pubmed - Toukan Y, Gur M, Bentur L. Negative pressure pulmonary edema following choking on a cookie. Pediatr Pulmonol. 2016;51(7):E25-27.
doi pubmed - Ginter D, Johnson KT, Venettacci O, Vanderlaan RD, Gilfoyle E, Mtaweh H. Case report: Foreign body aspiration requiring extracorporeal membrane oxygenation. Front Pediatr. 2023;11:1189722.
doi pubmed - Bohrer M, Long C, Thompson A, Veroukis S, Khaira G. Pediatric acute respiratory distress syndrome and tracheal injury in a patient requiring extracorporeal membrane oxygenation following cement aspiration: a case report. Crit Care Explor. 2023;5(9):e0969.
doi pubmed - Ayats-Vidal R, Vasquez-Perez A, Gallego-Diaz M, Rosell A, Valdesoiro-Navarrete L, Tazi-Mezalek R. Successful removal of distal persistent foreign body airway with CO2 cryotherapy in a child. Respir Med Case Rep. 2022;36:101594.
doi pubmed - David AP, Xu MJ, Rosbe KW, Meyer AK, Gesthalter YB, Chan DK. Cryoprobe retrieval of an airway foreign body: A case report and literature review. Int J Pediatr Otorhinolaryngol. 2019;125:79-81.
doi pubmed - Zhang L, Yin Y, Zhang J, Zhang H. Removal of foreign bodies in children's airways using flexible bronchoscopic CO2 cryotherapy. Pediatr Pulmonol. 2016;51(9):943-949.
doi pubmed - Han LL, Meng C, Zhang ZX, Tang XD, Ma J, Li CX. Clinical analysis of bronchoscope diagnosis and treatment for airway foreign body removal in pediatric patients. Ital J Pediatr. 2022;48(1):159.
doi pubmed - Shostak E. Foreign body removal in children and adults: review of available techniques and emerging technologies. AME Med J. 2018;3:75.
doi - Schramm D, Freitag N, Kotz K, Iglesias-Serrano I, Culebras-Amigo M, Koblizek V, Perez-Tarazona S, et al. Cryotherapy in the paediatric airway: Indications, success and safety. Respirology. 2022;27(11):966-974.
doi pubmed - Ding L, Su S, Chen C, Yao H, Xiao L. Tracheobronchial foreign bodies in children: experience from 1,328 patients in China. Front Pediatr. 2022;10:873182.
doi pubmed - Ciftci AO, Bingol-Kologlu M, Senocak ME, Tanyel FC, Buyukpamukcu N. Bronchoscopy for evaluation of foreign body aspiration in children. J Pediatr Surg. 2003;38(8):1170-1176.
doi pubmed - Wu Y, Zhang X, Lin Z, Ding C, Wu Y, Chen Y, Wang D, et al. Changes in the global burden of foreign body aspiration among under-5 children from 1990 to 2019. Front Pediatr. 2023;11:1235308.
doi pubmed - Romero BM, Vilchez-Bravo S, Hernandez-Arriaga G, Bueso-Pineda L, Franchi T, Tovani-Palone MR, Mejia CR. Factors associated with complications of foreign body ingestion and/or aspiration in children from a Peruvian hospital. Heliyon. 2023;9(2):e13450.
doi pubmed - Boufersaoui A, Smati L, Benhalla KN, Boukari R, Smail S, Anik K, Aouameur R, et al. Foreign body aspiration in children: experience from 2624 patients. Int J Pediatr Otorhinolaryngol. 2013;77(10):1683-1688.
doi pubmed - Cascade PN, Alexander GD, Mackie DS. Negative-pressure pulmonary edema after endotracheal intubation. Radiology. 1993;186(3):671-675.
doi pubmed - Bos LDJ, Ware LB. Acute respiratory distress syndrome: causes, pathophysiology, and phenotypes. Lancet. 2022;400(10358):1145-1156.
doi pubmed - Wick KD, Ware LB, Matthay MA. Acute respiratory distress syndrome. BMJ. 2024;387:e076612.
doi pubmed - Beitler JR, Malhotra A, Thompson BT. Ventilator-induced lung injury. Clin Chest Med. 2016;37(4):633-646.
doi pubmed - Chiang MC, Lin WS, Lien R, Chou YH. Reexpansion pulmonary edema following patent ductus arteriosus ligation in a preterm infant. J Perinat Med. 2004;32(4):365-367.
doi pubmed - Mahfood S, Hix WR, Aaron BL, Blaes P, Watson DC. Reexpansion pulmonary edema. Ann Thorac Surg. 1988;45(3):340-345.
doi pubmed - Sharma S, Madan K, Singh N. Fatal re-expansion pulmonary edema in a young adult following tube thoracostomy for spontaneous pneumothorax. BMJ Case Rep. 2013;2013:bcr2013010177.
doi pubmed - Simpson R, Myer Iv C, Siracusa C. Acute respiratory distress syndrome immediately following the removal of an aspirated foreign body. Respir Med Case Rep. 2020;29:100978.
doi pubmed - Gobbel WG, Jr. Experimental peanut oil pneumonia in rabbits. Am J Dis Child (1911). 1949;77(2):175-184.
doi pubmed - Zhang X, Li WX, Cai YR. A time series observation of Chinese children undergoing rigid bronchoscopy for an inhaled foreign body: 3,149 cases in 1991-2010. Chin Med J (Engl). 2015;128(4):504-509.
doi pubmed - Jackson C, Spencer WH. Arachidic Bronchitis. JAMA. 1919;73(9):672-674.
doi - Moslehi MA. Foreign body retrieval by using flexible cryoprobe in children. J Bronchology Interv Pulmonol. 2021;28(2):103-106.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
International Journal of Clinical Pediatrics is published by Elmer Press Inc.