| International Journal of Clinical Pediatrics, ISSN 1927-1255 print, 1927-1263 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Int J Clin Pediatr and Elmer Press Inc |
| Journal website https://ijcp.elmerpub.com |
Original Article
Volume 15, Number 1, March 2026, pages 16-25

Oral Health Status and Salivary Pepsin Levels in Children With Gastroesophageal Reflux Disease Surgery: A Postoperative Evaluation
Kubra Saga, d, Ayse Burusb, Cansu Ozsin Ozlera, Tutku Soyerc, Yasemin Bayazitb, Ozlem Boybeyic, Meryem Uzamis Tekciceka
aFaculty of Dentistry, Department of Pediatric Dentistry, Hacettepe University, 06100 Ankara, Turkey
bFaculty of Medicine, Department of Medical Biochemistry, Hacettepe University, 06100 Ankara, Turkey
cFaculty of Medicine, Department of Pediatric Surgery, Hacettepe University, 06100 Ankara, Turkey
dCorresponding Author: Kubra Sag, Faculty of Dentistry, Department of Pediatric Dentistry, Hacettepe University, 06100 Ankara, Turkey
Manuscript submitted May 28, 2025, accepted August 25, 2025, published online March 26, 2026
Short title: Oral Health in Children With GERD Surgery
doi: https://doi.org/10.14740/ijcp1009
| Abstract | ▴Top |
Background: Gastroesophageal reflux disease (GERD) is characterized by the impact of gastroesophageal reflux on daily life and function, leading to troublesome symptoms and/or complications. This study was designed to evaluate oral and dental health, salivary parameters, and salivary pepsin concentrations in children operated on for GERD and compare them to those of healthy children.
Methods: Data were gathered by a questionnaire. Assessment of oral health included evaluation of dental caries, filling and missing tooth status, periodontal health, dental erosion status, and salivary parameters such as salivary flow, pH, buffering capacity, and pepsin levels. Pepsin enzyme concentrations in saliva samples were analyzed by sandwich enzyme-linked immunosorbent assay (ELISA).
Results: The study enrolled 42 children in total, comprising 16 who underwent surgical operations due to GERD with a mean age of 7.19 ± 4.651 years and 26 healthy controls with a mean age of 8 ± 4.186 years. The study group comprised children previously diagnosed with GERD who had undergone surgery, while the control group included medically healthy children without systemic conditions. The mean decayed, missing, filled tooth/surface (dmft/dmfs) indexes of children in the operated for GERD group are statistically significantly lower. In contrast, plaque index and gingival index means are higher than those of healthy children. The salivary pepsin level was found to be 95.219 ± 154.250 pg/mL in the operated for GERD group and 104.923 ± 193.869 pg/mL in the healthy group (P = 0.803).
Conclusions: GERD is a significant health problem that may have an impact on oral and dental health status. As oral health status of children may be impaired in children with GERD, pediatric dentists should take part in the multidisciplinary team during the diagnosis, treatment, and control follow-up of these patients.
Keywords: Gastroesophageal reflux diseases; Oral health; Children; Pepsin; Saliva
| Introduction | ▴Top |
Gastroesophageal reflux, which refers to the passage of gastric contents into the esophagus, can be defined as gastroesophageal reflux disease (GERD) when it affects one’s daily life and functioning, causing troublesome symptoms and/or complications [1]. There is growing evidence indicating that several factors might raise the risk of GERD in infants and children. These include preterm birth, birth-related complications [2], genetic and epigenetic factors [3–5], nutritional disorders, obesity, congenital heart diseases, gastrointestinal system anomalies, and use of certain drugs (such as calcium channel blockers, diazepam, theophylline, and methylxanthines) [6–10].
GERD accompanied by symptoms has been reported to have a prevalence range of 0.2–18.8% in children and adolescents [11, 12]. It is thought that in GERD, gastric fluid reaching the extraesophageal tissues may be responsible for the damage observed in tissues outside the stomach. It is often the case that reflux attacks occur in the postprandial period after meals or at night. This can cause the stomach contents to reach the esophagus and upper tissues, potentially leading to damage [13, 14]. In cases where pharmacological approaches to GERD treatment have been unsuccessful in achieving the desired results, surgical options may be considered. This could be the case when there are also anatomical disorders, recurrent pulmonary infections, or growth and development disorders present [1, 15–19].
Pepsin is secreted as pepsinogen from chief cells in the fundus of the stomach and is an endopeptidase enzyme that plays a role in the breakdown of dietary proteins in the stomach into amino acids [20]. It might be suggested that the detection of pepsin enzyme in areas outside the stomach could be an indicator of a reflux episode [21–25].
Some studies have explored the potential relationship between GERD and oral and dental health [26, 27]. Typical oral findings in GERD include dental erosions, dental caries, oral mucosal erythema, dry mouth, bad breath, and burning sensation in the mouth [28, 29].
The objective of this study was to assess the oral health, specific salivary parameters, and salivary pepsin levels in children who underwent surgery for GERD and to compare the findings with those of healthy children.
| Materials and Methods | ▴Top |
Ethical concerns and design
The study was conducted between June 2022 and October 2023 after the approval of the Hacettepe University Non-Interventional Research Ethics Committee (2022/05/10). The study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration. The participants in the study were grouped into study and control groups. All eligible pediatric patients aged 0–18 years who underwent surgery for GERD at the Pediatric Surgery Department of the Faculty of Medicine, Hacettepe University, and whose families provided consent, were included in the study. GERD diagnosis in all patients was confirmed clinically and radiologically before surgery. In this group, pediatric patients who did not comply during oral examination and/or saliva collection were excluded. The control group consisted of children aged 0–18 years who were admitted to the Pediatric Dentistry Department of the dental faculty at the same university, for any reason and whose families gave their consent to participate. Children in the control group were excluded from the study if they had any systemic disease and did not cooperate during oral and dental health evaluation and saliva collection. In this study, “healthy” refers to children without GERD and neurological impairment. They were medically healthy individuals as reported by their parents, and this information was subsequently verified through the electronic medical records system.
Oral examination
In data collection processes, a questionnaire form developed for this study, which consisted of questions about the child’s nutrition and oral care habits, was used. The oral and dental health records were written on examination record sheets. The oral hard and soft tissues and teeth were examined with a mouth mirror and a ball-tipped periodontal probe under the light of a dental unit. Dental caries were recorded according to the decayed, missing, filled tooth/surface in both primary and permanent tooth (dmft/s and DMFT/S, respectively) indices for primary and permanent teeth, respectively [30]. The Gingival Index (GI) and Plaque Index (PI) [31] were used to assess gingival health and dental plaque status. In these indices, Ramfjord teeth, known as the partial periodontal recording system, were used due to ease of application in young age groups and individuals with special health needs [32, 33]. The presence of dental erosion was evaluated with the Basic Erosive Wear Examination (BEWE) index [34]. Abbreviations and definitions of the indices employed to assess oral health are presented in Table 1. All examinations were performed by one research assistant in pediatric dentistry (KS); to ensure the reliability and reproducibility of the clinical assessments, specific training on the application of all World Health Organization (WHO) indices was provided by a professor of pediatric dentistry with 35 years of professional experience. Before the initiation of data collection, intra-examiner calibration between the professor and the examining dentist was performed, yielding a Cohen’s kappa coefficient of 0.92, indicating excellent agreement. In addition, the dentition stage (primary, mixed, or permanent) was recorded for each child.
 Click to view | Table 1. Abbreviations and Definitions of the Indices Employed to Assess Oral Health |
Saliva collection/assessment
The saliva samples of children who could be orally fed and able to cooperate were collected between 9:00 and 10:00 a.m. before any food or water intake, tooth brushing, or mouth rinsing. In children who were not fed orally, saliva was collected just before their regular feeding. For saliva collection, three Salivette rolls (Sarstedt, Numbrecht, Germany) were placed in the mouth for 5 min without stimulation: two positioned at the orifices of the Stensen ducts, one to the mouth floor where ducts from the Wharton and sublingual glands open. Samples were then transferred into particular centrifugation tubes and centrifuged at 1,000 × g for 2 min to obtain supernatants. The saliva flow rate was recorded in mL/min. pH and buffering capacity were assessed using the Saliva-Check Buffer Kit (GC Corporation, Tokyo, Japan). The collected saliva samples for enzyme-linked immunosorbent assay (ELISA) analysis were stored at −20 °C.
Pepsin saliva measurement
Pepsin levels in saliva samples were quantified by using a sandwich ELISA [35] method with a commercially available Human Pepsin ELISA kit (Elabscience, Houston, USA), designed to detect concentrations within the range of 62.50–4,000 pg/mL. Samples falling below the lower limit of detection were reported as 0 pg/mL. All the experimental procedures were performed following the manufacturer’s instructions. Briefly, 100 µL samples were added to the wells of a precoated 96-well plate and incubated for 90 min at 37 °C. Then, wells were washed and incubated with biotinylated secondary antibody for 60 min at 37 °C. After another washing procedure, wells were incubated with TMB substrate solution for 15 min at 37 °C. The enzymatic reaction was stopped by adding stop solution, and the absorbance of each well was immediately measured at 450 nm using a microplate reader. A standard curve generated from known concentrations of pepsin standards was used to calculate the concentration of pepsin in each sample (pg/mL). Each assay was performed in duplicate.
Statistical assessment and data analysis
The recording of data and statistical analyses in the research was carried out by the authors. All statistical analyses were performed using the IBM SPSS 23.0 (SPSS Inc., Chicago, IL, USA) software package. For descriptive statistics, frequency and percentage were calculated for categorical variables, and mean, standard deviation (SD), median, minimum, and maximum values were calculated for numerical variables. Numerical variables were considered as parametric data if normality tests were met, and an independent samples t-test was used to compare two independent groups. In cases where normality was not met and non-parametric data were present, the Mann-Whitney U test was used for comparing two independent groups. Chi-square test was used for comparing categorical variables, and Fisher’s exact test or exact test was used when necessary. Pearson correlation test was applied to evaluate relationships between numerical values in parametric cases, while Spearman’s correlation test was applied in non-parametric cases. The level of statistical significance was set at P < 0.05.
| Results | ▴Top |
Sixteen children aged 0–14 years who underwent Nissen fundoplication for GERD participated in the study, including 10 boys (62.5%) and 6 girls (37.5%), with a mean age of 7.19 ± 4.651 years. In the healthy group, there were 26 children aged 0–14 years, including 16 boys (61.5%) and 10 girls (38.5%), with a mean age of 8 ± 4.186 years. The gender and age distribution between the operated for GERD group and the healthy group were evaluated, and no statistically significant difference was found between the groups (gender; P = 0.950; age; P = 0.576).
In the study, 56.3% (n = 9) of the children in the operated for GERD group were not fed orally. One of these children was fed through a nasogastric tube (NG), while the others were fed through a percutaneous endoscopic gastrostomy (PEG). According to the parents, 81.3% (n = 13) of the children in the operated for GERD group had difficulty in chewing. A total of 68.8% of children in the operated for GERD group exhibited neurological impairment. Furthermore, it was determined that 72.7% of these children were fed only through gastrostomy tubes.
According to the results, it was reported by the parents that 50% of the children in the operated for GERD group, whereas 84.6% of the children in the healthy group had previously visited a dentist. Additionally, it was found that half (n = 8) of the children in the operated for GERD group did not brush their teeth, and approximately one-third (n = 5) had their teeth brushed by their parents. The children in the group who failed to brush their teeth were those who were not fed orally. In the healthy group, it was learned that 7.7% (n = 2) of children did not brush their teeth, while 73.1% (n = 19) brushed their teeth themselves.
The data evaluating the oral health of children participating in the study are presented in Table 2. The dmft and dmfs scores of children in the healthy group were statistically significantly higher than those in operated for GERD group, while the PI and GI scores of children in the operated for GERD group were significantly higher (P < 0.05). In the group of children who underwent surgery for GERD, the distribution across dentition types was as follows: six children in primary, eight children in mixed, and two in permanent dentition. Within the healthy group, eight children were in primary, fourteen in mixed, and four in permanent dentition.
Click to view | Table 2. Distribution Statistics of the Indices Indicating the Oral Health Status and Salivary Parameters of the Children in the Operated for GERD and Healthy Groups Participating in the Study |
Erosive lesions in dental hard tissues were detected in 50% of the children in the operated for GERD group compared to 38.5% in the healthy group. The mean total BEWE score was 2.93 ± 3.362 for the operated for GERD group and 0.77 ± 1.21 for the healthy group. The observed difference between the groups was not statistically significant (P = 0.094). The region with the highest mean BEWE score in both groups was the anterior maxillary region. In addition, the mean BEWE scores in the maxillary anterior region were significantly higher in children of operated for GERD group (P = 0.046).
The unstimulated saliva sample parameters are presented in Table 2. No statistically significant differences were observed between the operated for GERD and healthy groups in terms of salivary pH, buffering capacity, salivary flow rate (mL/min), and pepsin concentrations (P > 0.05). In addition, in both primary and permanent dentition (dmft, dmfs, DMFT, and DMFS) indices median (IQR) scores were 0 (1 to 2) in the operated for GERD group in children who were not fed orally.
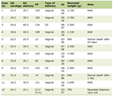
In the operated for GERD group, the mean interval between fundoplication surgery and the study assessment was 24.8 ± 13.7 months. The age at which children underwent surgery for GERD ranged from 1 to 13 years, with the mean operation age of 5.5 ± 4.397 years. Based on the time elapsed since the surgical operation for GERD, the distribution of the group was as follows: 0–6 months (12.5%), 13–24 months (43.8%), 25–36 months (25.0%), and more than 36 months (18.8%).
In the operated for GERD group, the results of correlation analysis are shown in Tables 3 and 4. Similar to the operated for GERD group, a strong positive correlation was observed between dmft and dmfs, and between DMFT and DMFS in the healthy group. In addition, as salivary pepsin concentrations increased in this group, the total BEWE (r = 0.461; P = 0.018) and the PI scores (r = 0.573; P = 0.003) also increased. This relationship was found to be statistically significant, indicating a moderate positive correlation (Table 4).
Click to view | Table 3. The Relationship Between Some Salivary Parameters of Children in the GERD Group Participating in the Study |
Click to view | Table 4. The Relationship Between Some Oral Dental Health Findings of the Children in the GERD Group Participating in the Study (Spearman’s rho) |
Table 5 presents a comparative overview of oral health indices and salivary parameters between children who underwent surgery for GERD and the control group, highlighting significantly lower dmft/dmfs, higher PI, and GI scores in the operated group, while no significant differences were observed in salivary parameters.
Click to view | Table 5. Comparison of Oral Health Indices and Salivary Parameters Between Children Operated for GERD and Healthy Controls |
| Discussion | ▴Top |
Previous research has evaluated the success of surgical intervention for GERD in children, primarily through survey-based outcomes related to GERD symptom status and quality of life for both the children and their families. However, no studies have been found that examine the postoperative oral health of children who have undergone surgical treatment for GERD [36–38].
In this study, it is considered that the oral health of children with neurological defects, who constitute 68.8% of the operated for GERD group, is affected by their condition. These children frequently encounter acidic gastric fluids in their oral soft and hard tissues as a consequence of GERD. Furthermore, the neurological defects characteristic of this group not only lead to dysfunctions of the oro-muscular system and salivary glands but also compromise mastication, swallowing efficiency, and oral clearance. These impairments, coupled with reduced motor coordination and limited self-care ability, substantially hinder effective oral hygiene practices and increase the vulnerability of these children to dental plaque accumulation and subsequent oral diseases [39, 40]. These factors may cause poor oral health in this population. Furthermore, in light of the prolonged hospitalizations of these children with multiple comorbidities, as well as the significant involvement and burnout of parents in their care [41, 42], it is imperative to regularly take care of parents about their children’s oral health. Promoting awareness through educational programs and ensuring regular oral health check-ups are crucial. In this context, since oral health is an inseparable component of overall health, it is of particular significance in children with neurological impairments and GERD that pediatric dentists are included in the multidisciplinary teams responsible for diagnosis, treatment, and long-term follow-up.
Hidas et al reported that children who were fed via gastrostomy tubes exhibited a significantly higher prevalence of dental calculus and a lower incidence of dental caries compared to a control group of healthy children [43]. The absence of cariogenic nutritional substrates may account for the low caries indices observed in children who are not orally fed. In the study conducted by Kumar et al [29] on 51 pediatric patients with GERD, 17.65% of the children were reported to have good oral hygiene, 23.53% had moderate oral hygiene, and 58.85% had poor oral hygiene. Our research demonstrated that the operated for GERD group were unable to perform self-brushing due to the presence of concomitant medical conditions, such as neurological disorders. Consequently, their oral hygiene was maintained by their parents. In the group of children with GERD who had undergone surgery, parents reported that the majority of children with neurological defects did not have their teeth brushed. It is imperative to give regular education by dentists to enhance parents’ knowledge, awareness, and habits in this regard.
Our results revealed that the dmft and dmfs indices were statistically significantly higher in the healthy group compared to the operated for GERD group. Some studies in the literature have found that children with GERD experience higher caries, suggesting that the acid resulting from GERD creates a favorable environment for aciduric Streptococcus mutans in the mouth and contributes to the formation of caries [44]. In our study, the children who underwent surgical operations due to GERD had their operations at an early age, around 5.5 years old. This protected the oral environment from acidic gastric fluids. Additionally, 56.3% of these children were not fed orally. The lower caries scores observed in the operated for GERD group may be attributable to factors such as non-oral feeding, earlier age at surgery, and diet modifications that reduce cariogenic exposure. The early age at which surgery was performed in the GERD group may have limited the potential impact of erosion on enamel surfaces.
The results of the study demonstrated that the PI and GI values observed in the operated for GERD group were statistically significantly higher in comparison to the healthy control group. These values were observed to be higher in children who were not fed orally in the operated for GERD group. The fact that half of the group that had GERD surgery did not brush their teeth may have contributed to the worsening of the current situation. Based on the available data, it is postulated that the accumulation of dental plaque and calculus in the operated for GERD group, coupled with the presence of various swallowing and movement disorders, has an adverse impact on periodontal health. Higher PI and GI scores were more closely associated with neurological impairment and inadequate oral hygiene, representing modifiable risk factors. Research findings suggest that children who are fed through a gastrostomy tube exhibit a higher accumulation of dental calculus compared to healthy children, which may potentially lead to aspiration pneumonia in these children [43, 45].
Prevalence of dental erosion in pediatric populations ranges from 15.1% to 82.3% [29, 46–49]. A meta-analysis published in 2022 reported the prevalence of dental erosion in preschool children to be 38.38% [50]. Similarly, in our study, signs of tooth erosion were observed in 38.5% of the children in the healthy group. In addition, several studies in both children and adults have shown a significant association between GERD and dental erosion [28, 44, 51–53]. The differences between the data obtained in our study and the results of other studies may be due to variations in the indices used to evaluate dental erosion, differences in age groups, and sample sizes. In addition, in our study, the maxillary anterior teeth were found to be most affected by erosive tooth wear in both groups, which supports the findings of Shaik et al [49, 54]. In our study, elevated BEWE scores, however, appear to reflect prior long-term reflux exposure and are less likely to be reversible following surgery.
A study conducted in Israel examined the oral health status of children who were fed via gastrostomy tubes. The findings indicated that these children exhibited higher levels of dental calculus, fewer dental caries, and lower levels of Streptococcus mutans and Lactobacillus in their saliva [43]. The study reported that children with neurological defects who were fed via gastrostomy tubes exhibited no dmft/DMFT scores, a finding that aligns with the results of Cardona-Soria’s research [45]. Our findings are consistent with earlier studies, which likewise demonstrated zero dmft/DMFT scores in children with GERD who were not fed orally. In children who are not orally fed, the absence of fermentable carbohydrates in the oral environment may limit the acid production of bacteria, thereby inhibiting the development of caries.
Singh et al reported mean (± SD) unstimulated salivary pH as 7.2 (± 0.24) and buffering capacity as 6.07 (± 0.53) in 80 healthy children aged 4 to 8 years [55]. Pachori et al found mean saliva pH values of 7.23 (± 0.18) and buffering capacity of 9.34 (±1.507) in 50 healthy children aged 8 to 12 years [56]. The study published by Akleyin et al in 2022 recorded salivary pH values as 6.89 (± 0.44) and buffering capacity as 7.6 (± 2.27) in 10 children [57]. Preethi et al found mean (± SD) salivary pH as 7.07 (± 0.43) and a buffering capacity of 5.32 (± 0.40) in their study of 120 participants aged 7 to 14 years. These results are similar to those found in our current study [58]. The flow rates of unstimulated saliva in healthy children aged 4 to 12 years were reported by Lopez et al [59] as 0.25 (± 0.13) mL/min, by Animireddy et al [60] as 0.43 (± 0.09) mL/min, and by O’Sullivan et al [61] as 0.44 (± 0.03) mL/min. On the other hand, Forcella et al [62] reported a salivary flow rate of 0.76 mL/min in children aged 6 to 15 years.
Reasons for the variable results of salivary parameters measured in studies of younger samples include difficulties in obtaining cooperation during the saliva collection procedure in the pediatric age group, differences in saliva collection methods, uncertainty in the timing of saliva collection according to circadian rhythms, wide age ranges within the pediatric sample group, investigator interpretation of the evaluation kits, and differences in adherence to manufacturers’ instructions during the measurement process [61].
The presence of the enzyme pepsin in the esophagus and supra-esophageal tissues, outside the stomach, is considered an indicator of a GER episode [63]. Researchers use salivary pepsin levels to diagnose GERD and evaluate the success of treatments [25, 21, 64–69]. In our study, we employed an ELISA test with a sensitivity of 37.5 pg/mL for the quantitative analysis of pepsin, which was not utilized in other studies. This decision was based on the proven success of surgical treatment in the operated for GERD group and the anticipation that physiological GER episodes in healthy children would carry small amounts of pepsin into the oral cavity.
In a study conducted on the pediatric population, Fortunato et al employed the sandwich ELISA method to analyze pepsin levels in samples from children with GERD and a control group. The results indicated that the mean pepsin levels in the GERD group were 22 ± 540 ng/mL, while the control group exhibited levels of 36 ± 210 ng/mL [70]. In a study conducted by Mozheiko et al (2023), a similar sandwich ELISA method was employed, and pepsin levels in the GERD group were reported to be 456.8 ± 56.9 pg/mL in saliva, while in the healthy group, they were 28.5 ± 11.6 pg/mL [71]. Salivary pepsin concentration was analyzed using the sandwich ELISA method. In our study, the average salivary pepsin concentration in the operated for GERD group was found to be 95.219 ± 154.250 pg/mL, whereas it was 104.923 ± 193.869 pg/mL in the healthy group. The average pepsin concentration in the operated for GERD group was lower than that in the healthy group, and there was no statistically significant difference in pepsin concentrations between the two groups. The data obtained from our study indicated that, despite the meantime of 24.8 ± 13.7 months having elapsed since the surgical treatment of GERD, the operated for GERD group exhibited lower concentrations of the pepsin enzyme compared to the healthy control group. This finding indicates that salivary pepsin concentrations may decline following Nissen fundoplication. However, comparative studies evaluating pre- and post-preparative pepsin levels are needed to have a firm conclusion.
The literature includes studies examining oral health findings related to GERD across a wide age range [29]. Additionally, researchers have investigated salivary pepsin concentrations both before and after surgical intervention for GERD, highlighting its potential as a reflux biomarker [72]. To the best of our knowledge, our study represents the inaugural descriptive research in the literature to provide comprehensive data on the oral health status of pediatric patients following surgical intervention for GERD. The study comprises a comprehensive survey of the child and their family history, an in-depth oral health examination utilizing a range of indices, and an analysis of multiple standardized salivary parameters that could impact oral health.
The associations between pepsin levels and oral parameters observed in our study are noteworthy. Specifically, salivary pepsin concentrations showed a positive correlation with both BEWE and PI scores, suggesting a potential link between reflux severity and oral health deterioration. Most correlations were not statistically significant, likely reflecting limited sample size. The significant correlation between dmft and dmfs is expected because both capture caries experience. It is noteworthy that the acidic gastric contents—responsible for irreversible erosion of dental hard tissues—can be weakly associated with the presence of pepsin enzyme in the oral cavity, which functions as a biomarker of reflux. The positive associations between salivary pepsin, BEWE, and PI warrant confirmation in larger cohorts. These findings highlight the need for future studies with larger samples and prospective designs to clarify the clinical implications of salivary pepsin as a biomarker in pediatric patients.
The healthy control group in this study consisted of children admitted for any reason to the pediatric dental clinic. Although 3% were referred due to caries, this finding appears consistent with national epidemiological data indicating a high prevalence of dental caries among Turkish children. According to the 2018 Turkish National Oral Health Survey, caries prevalence was 66.2% in 5 years old, 54.7% in 12 years old, and 69.4% in 15 years old children [73]. These figures suggest that the “healthy” group reflects the general pediatric population in Turkey, thereby supporting the representativeness of the control sample. The main limitations of this study include the limited sample size, insufficient cooperation of young children or those with medical problems during oral examinations and saliva collection, and the use of a dental erosion index that does not differentiate between primary and permanent teeth. In addition, for some salivary parameter evaluations, patient-side methods were used instead of laboratory analyses. Furthermore, patients in the operated for GERD group underwent surgery at different times until 2023, resulting in different durations since their surgical intervention. Therefore, salivary parameters and oral health status could not be directly correlated with the surgical procedure. There is a need for studies that evaluate pre- and postoperative conditions to assess the impact of surgical intervention on GERD symptoms. Finally, due to the limited number of studies on this topic, there are few resources available to compare and evaluate research findings.
Conclusions
This study evaluated the oral and dental health status, salivary parameters, and pepsin concentration of 16 pediatric patients who underwent surgical treatment for GERD and compared them with 26 healthy children of similar age and gender characteristics. In the operated for GERD group, the mean dmft/dmfs and index were lower, while the mean PI and GI were higher compared to healthy children, and these differences were statistically significant (P < 0.05). In addition, 56.3% of the children in the operated for GERD group were not orally fed. In the non-orally fed children in this group, the dmft/dmfs and DMFT/DMFS indices were zero. The mean pepsin concentration in the operated for GERD group was lower than in the healthy group, but there was no statistically significant difference in pepsin concentration between the two groups.
Oral health is an integral part of overall health. Especially in conditions where neurological defects and GERD are observed, it is essential to include pediatric dentists in the team that diagnose, treat, and monitor these conditions. This collaborative approach enables early diagnosis and treatment planning in dentistry. Therefore, these children should be referred to dentists by their physicians at an early stage. In these cases, a holistic approach to diagnosis and treatment is crucial. Within a multidisciplinary framework, the pediatric dentist should be included in this group. More comprehensive studies are needed to evaluate the impact of GERD on oral health.
Acknowledgments
The authors would also like to thank the participants who agreed to be part of this study.
Financial Disclosure
This study was supported by the Scientific Research Projects Coordination Unit, Hacettepe University, Ankara, Turkey (Project code: TDH-2022-20233).
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Ethics approval and consent to participate in the study were based on the approval of Hacettepe University’s Non-Interventional Clinical Research Ethics Committee (2022/05/10) and written consent of the parents.
Author Contributions
Concept: KS, AB, COO, TS, YB, OB, MUT; data collection or processing: KS, AB, COO, MUT; analysis or interpretation: KS, COO, MUT; literature search: KS, COO, MUT; writing: KS, AB, COO, MUT; project supervision: MUT. All authors reviewed the manuscript.
Data Availability
The data that support the findings of this study are available on request from the corresponding author.
| References | ▴Top |
- Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, Gupta S, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the north american society for pediatric gastroenterology, hepatology, and nutrition and the european society for pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr. 2018;66(3):516-554.
doi pubmed - Dahlen HG, Foster JP, Psaila K, Spence K, Badawi N, Fowler C, Schmied V, et al. Gastro-oesophageal reflux: a mixed methods study of infants admitted to hospital in the first 12 months following birth in NSW (2000-2011). BMC Pediatr. 2018;18(1):30.
doi pubmed - Hu FZ, Preston RA, Post JC, White GJ, Kikuchi LW, Wang X, Leal SM, et al. Mapping of a gene for severe pediatric gastroesophageal reflux to chromosome 13q14. JAMA. 2000;284(3):325-334.
doi pubmed - Kaz AM, Grady WM, Stachler MD, Bass AJ. Genetic and epigenetic alterations in barrett's esophagus and esophageal adenocarcinoma. Gastroenterol Clin North Am. 2015;44(2):473-489.
doi pubmed - Carroll AE, Garrison MM, Christakis DA. A systematic review of nonpharmacological and nonsurgical therapies for gastroesophageal reflux in infants. Arch Pediatr Adolesc Med. 2002;156(2):109-113.
doi pubmed - Arcos-Machancoses JV, Ruiz Hernandez C, Martin de Carpi J, Pinillos Pison S. A systematic review with meta-analysis of the prevalence of gastroesophageal reflux in congenital diaphragmatic hernia pediatric survivors. Dis Esophagus. 2018;31(6).
doi pubmed - Kawahara H, Tazuke Y, Soh H, Usui N, Okuyama H. Characteristics of gastroesophageal reflux in pediatric patients with neurological impairment. Pediatr Surg Int. 2017;33(10):1073-1079.
doi pubmed - Kim S, Koh H, Lee JS. Gastroesophageal reflux in neurologically impaired children: What are the risk factors? Gut Liver. 2017;11(2):232-236.
doi pubmed - Blanco FC, Davenport KP, Kane TD. Pediatric gastroesophageal reflux disease. Surg Clin North Am. 2012;92(3):541-558, viii.
doi pubmed - Leung AK, Hon KL. Gastroesophageal reflux in children: an updated review. Drugs Context. 2019;8:212591.
doi pubmed - Landau DA, Goldberg A, Levi Z, Levy Y, Niv Y, Bar-Dayan Y. The prevalence of gastrointestinal diseases in Israeli adolescents and its association with body mass index, gender, and Jewish ethnicity. J Clin Gastroenterol. 2008;42(8):903-909.
doi pubmed - Gunasekaran TS, Dahlberg M. Prevalence of gastroesophageal reflux symptoms in adolescents: is there a difference in different racial and ethnic groups? Dis Esophagus. 2011;24(1):18-24.
doi pubmed - Bredenoord AJ, Pandolfino JE, Smout AJ. Gastro-oesophageal reflux disease. Lancet. 2013;381(9881):1933-1942.
doi pubmed - Orr WC. Review article: sleep-related gastro-oesophageal reflux as a distinct clinical entity. Aliment Pharmacol Ther. 2010;31(1):47-56.
doi pubmed - Gulerman F. Cocuklarda Gastroozofageal Reflu Hastaligi. Guncel Gastroenteroloji. 2015.
- De Backer A. Surgical options to treat GERD. In: Vandenplas Y, editor. Gastroesophageal Reflux in Children. Cham: Springer International Publishing; 2022. p. 361-370.
- Sullivan PB. Gastrostomy feeding in the disabled child: when is an antireflux procedure required? Arch Dis Child. 1999;81(6):463-464.
doi pubmed - Aumar M, Lalanne A, Guimber D, Coopman S, Turck D, Michaud L, Gottrand F. Influence of percutaneous endoscopic gastrostomy on gastroesophageal reflux disease in children. J Pediatr. 2018;197:116-120.
doi pubmed - Diamond IR, Mah K, Kim PC, Bohn D, Gerstle JT, Wales PW. Predicting the need for fundoplication at the time of congenital diaphragmatic hernia repair. J Pediatr Surg. 2007;42(6):1066-1070.
doi pubmed - Li Y, Xu G, Zhou B, Tang Y, Liu X, Wu Y, Wang Y, et al. Effects of acids, pepsin, bile acids, and trypsin on laryngopharyngeal reflux diseases: physiopathology and therapeutic targets. Eur Arch Otorhinolaryngol. 2022;279(6):2743-2752.
doi pubmed - Dy F, Amirault J, Mitchell PD, Rosen R. Salivary pepsin lacks sensitivity as a diagnostic tool to evaluate extraesophageal reflux disease. J Pediatr. 2016;177:53-58.
doi pubmed - Hayat JO, Gabieta-Somnez S, Yazaki E, Kang JY, Woodcock A, Dettmar P, Mabary J, et al. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut. 2015;64(3):373-380.
doi pubmed - Sereg-Bahar M, Jerin A, Jansa R, Stabuc B, Hocevar-Boltezar I. Pepsin and bile acids in saliva in patients with laryngopharyngeal reflux - a prospective comparative study. Clin Otolaryngol. 2015;40(3):234-239.
doi pubmed - Fortunato JE, D'Agostino RB, Jr., Lively MO. Pepsin in saliva as a biomarker for oropharyngeal reflux compared with 24-hour esophageal impedance/pH monitoring in pediatric patients. Neurogastroenterol Motil. 2017;29(2).
doi pubmed - Kahrilas PJ, Kia L. Pepsin: a silent biomarker for reflux aspiration or an active player in extra-esophageal mucosal injury? Chest. 2015;148(2):300-301.
doi pubmed - Petruzzi M, Lucchese A, Campus G, Crincoli V, Lauritano D, Baldoni E. Oral stigmatic lesions of gastroesophageal reflux disease (GERD). Rev Med Chil. 2012;140(7):915-918.
doi pubmed - Tolia V, Vandenplas Y. Systematic review: the extra-oesophageal symptoms of gastro-oesophageal reflux disease in children. Aliment Pharmacol Ther. 2009;29(3):258-272.
doi pubmed - Ignat A, Burlea M, Lupu VV, Paduraru G. Oral manifestations of gastroesophageal reflux disease in children. Rom J Oral Rehabil. 2017;9:40-43.
- Sarath Kumar KS, Mungara J, Venumbaka NR, Vijayakumar P, Karunakaran D. Oral manifestations of gastroesophageal reflux disease in children: A preliminary observational study. J Indian Soc Pedod Prev Dent. 2018;36(2):125-129.
doi pubmed - Merchan MT, Ismail AI. 14 - Measurement and Distribution of Dental Caries. In: Mascarenhas AK, Okunseri C, Dye BA, editors. Burt and Eklund's Dentistry, Dental Practice, and the Community (Seventh Edition). St. Louis: W.B. Saunders; 2021. p. 154-170.
- Fischman SL. Current status of indices of plaque. J Clin Periodontol. 1986;13(5):371-374, 379-380.
doi pubmed - Fleiss JL, Park MH, Chilton NW, Alman JE, Feldman RS, Chauncey HH. Representativeness of the "Ramfjord teeth" for epidemiologic studies of gingivitis and periodontitis. Community Dent Oral Epidemiol. 1987;15(4):221-224.
doi pubmed - Ramfjord SP. Indices for prevalence and incidence of periodontal disease. 1959.
- Bartlett D, Ganss C, Lussi A. Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008;12(Suppl 1):S65-68.
doi pubmed - Tham R, Bowatte G, Dharmage SC, Tan DJ, Lau MX, Dai X, Allen KJ, et al. Breastfeeding and the risk of dental caries: a systematic review and meta-analysis. Acta Paediatr. 2015;104(467):62-84.
doi pubmed - Ozcakir E. Laparoskopik nissen fundoplikasyonu yapilan gastroozofageal reflu hastalikli cocuklarin yasam kalitesi olcegi ile degerlendirilmesi. Bursa Uludag University (Turkey). 2010.
- Pacilli M, Eaton S, McHoney M, Kiely EM, Drake DP, Curry JI, Lindley KJ, et al. Four year follow-up of a randomised controlled trial comparing open and laparoscopic Nissen fundoplication in children. Arch Dis Child. 2014;99(6):516-521.
doi pubmed - Pilli S, Jiwane A, Krishnan U. Quality of life in children who have undergone fundoplication surgery for the treatment of gastroesophageal reflux disease: a review of literature. Dis Esophagus. 2017;30(5):1-5.
doi pubmed - Benfer KA, Weir KA, Bell KL, Ware RS, Davies PS, Boyd RN. Oropharyngeal dysphagia in preschool children with cerebral palsy: oral phase impairments. Res Dev Disabil. 2014;35(12):3469-3481.
doi pubmed - Calis EA, Veugelers R, Sheppard JJ, Tibboel D, Evenhuis HM, Penning C. Dysphagia in children with severe generalized cerebral palsy and intellectual disability. Dev Med Child Neurol. 2008;50(8):625-630.
doi pubmed - Mugno D, Ruta L, D'Arrigo VG, Mazzone L. Impairment of quality of life in parents of children and adolescents with pervasive developmental disorder. Health Qual Life Outcomes. 2007;5:22.
doi pubmed - Ersoy AF, Bulus S. Engelli Cocugu Olan Annelerde Tukenmislik: Nitel Bir Calisma. Turkiye Sosyal Arastirmalar Dergisi. 2019;23(3):764-781.
- Hidas A, Cohen J, Beeri M, Shapira J, Steinberg D, Moskovitz M. Salivary bacteria and oral health status in children with disabilities fed through gastrostomy. Int J Paediatr Dent. 2010;20(3):179-185.
doi pubmed - Linnett V, Seow WK, Connor F, Shepherd R. Oral health of children with gastro-esophageal reflux disease: a controlled study. Aust Dent J. 2002;47(2):156-162.
doi pubmed - Cardona-Soria S, Cahuana-Cardenas A, Rivera-Baro A, Miranda-Rius J, Martin de Carpi J, Brunet-Llobet L. Oral health status in pediatric patients with cerebral palsy fed by oral versus enteral route. Spec Care Dentist. 2020;40(1):35-40.
doi pubmed - Li Y, Wang Z, Fang M, Tay FR, Chen X. Association between gastro-oesophageal reflux disease and dental erosion in children: a systematic review and meta-analysis. J Dent. 2022;125:104247.
doi pubmed - Alves LS, Brusius CD, Dame-Teixeira N, Maltz M, Susin C. Dental erosion among 12-year-old schoolchildren: a population-based cross-sectional study in South Brazil. Int Dent J. 2015;65(6):322-330.
doi pubmed - Brusius CD, Alves LS, Susin C, Maltz M. Dental erosion among South Brazilian adolescents: a 2.5-year longitudinal study. Community Dent Oral Epidemiol. 2018;46(1):17-23.
doi pubmed - Shaik R, Yogesh PNARS, Heralgi GKGR. Erosive tooth wear among 3-6 year old kindergarten children in Nellore District of Andhra Pradesh. J Res Adv Dent. 2018;8:114-124.
- Yip K, Lam PPY, Yiu CKY. Prevalence and associated factors of erosive tooth wear among preschool children-a systematic review and meta-analysis. Healthcare (Basel). 2022;10(3):491.
doi pubmed - Farahmand F, Sabbaghian M, Ghodousi S, Seddighoraee N, Abbasi M. Gastroesophageal reflux disease and tooth erosion: a cross-sectional observational study. Gut Liver. 2013;7(3):278-281.
doi pubmed - Lechien JR, Calvo-Henriquez C, Chiesa-Estomba CM, Barillari MR, Trozzi M, Meucci D, Peer S, et al. Reflux and dental disorders in the pediatric population: A systematic review. Int J Pediatr Otorhinolaryngol. 2020;136:110166.
doi pubmed - De Oliveira PA, Paiva SM, De Abreu MH, Auad SM. Dental erosion in children with gastroesophageal reflux disease. Pediatr Dent. 2016;38(3):246-250.
pubmed - Carvalho TS, Lussi A, Jaeggi T, Gambon DL. Erosive tooth wear in children. Monogr Oral Sci. 2014;25:262-278.
doi pubmed - Singh S, Sharma A, Sood PB, Sood A, Zaidi I, Sinha A. Saliva as a prediction tool for dental caries: An in vivo study. J Oral Biol Craniofac Res. 2015;5(2):59-64.
doi pubmed - Pachori A, Kambalimath H, Maran S, Niranjan B, Bhambhani G, Malhotra G. Evaluation of changes in salivary pH after intake of different eatables and beverages in children at different time intervals. Int J Clin Pediatr Dent. 2018;11(3):177-182.
doi pubmed - Akleyin E, Sariyildiz CO, Yavuz I, Toptanci IR. Saliva analysis in children with active caries before and after dental treatment. Dental Journal (Majalah Kedokteran Gigi). 2022;55(3):120-124.
- Preethi BP, Reshma D, Anand P. Evaluation of flow rate, pH, buffering capacity, calcium, total proteins and total antioxidant capacity levels of saliva in caries free and caries active children: an in vivo study. Indian J Clin Biochem. 2010;25(4):425-428.
doi pubmed - Lopez ME, Colloca ME, Paez RG, Schallmach JN, Koss MA, Chervonagura A. Salivary characteristics of diabetic children. Braz Dent J. 2003;14(1):26-31.
doi pubmed - Animireddy D, Reddy Bekkem VT, Vallala P, Kotha SB, Ankireddy S, Mohammad N. Evaluation of pH, buffering capacity, viscosity and flow rate levels of saliva in caries-free, minimal caries and nursing caries children: An in vivo study. Contemp Clin Dent. 2014;5(3):324-328.
doi pubmed - O'Sullivan EA, Curzon ME. Salivary factors affecting dental erosion in children. Caries Res. 2000;34(1):82-87.
doi pubmed - Forcella L, Filippi C, Waltimo T, Filippi A. Measurement of unstimulated salivary flow rate in healthy children aged 6 to 15 years. Swiss Dent J. 2018;128(12):962-967.
doi pubmed - Fisher J, Porter G, Graham S, Ziaras C, Woodcock AD, Dettmar PW. Tooth erosion and the role of pepsin reflux. J Clin Adv Dent. 2020;4:9-14.
- Knight J, Lively MO, Johnston N, Dettmar PW, Koufman JA. Sensitive pepsin immunoassay for detection of laryngopharyngeal reflux. Laryngoscope. 2005;115(8):1473-1478.
doi pubmed - Yu L, Li R, Du L, Zhao Y. The diagnostic value of pepsin concentration in saliva for laryngopharyngeal reflux disease. Eur Arch Otorhinolaryngol. 2022;279(12):5783-5789.
doi pubmed - Yadlapati R, Kaizer A, Greytak M, Ezekewe E, Simon V, Wani S. Diagnostic performance of salivary pepsin for gastroesophageal reflux disease. Dis Esophagus. 2021;34(4).
doi pubmed - Rajab YS, Zaidan TF. Evaluation of salivary pepsin levels and dental erosion in patients with gastroesophageal reflux disease. Cureus. 2023;15(2):e34744.
doi pubmed - Farhath S, He Z, Saslow J, Soundar S, Amendolia B, Bhat V, Pyon K, et al. Detection of pepsin in mouth swab: correlation with clinical gastroesophageal reflux in preterm infants. J Matern Fetal Neonatal Med. 2013;26(8):819-824.
doi pubmed - Lechien JR, Bobin F. Saliva pepsin measurements in the detection of gastroesophageal reflux disease in laryngopharyngeal reflux patients: a cohort study. Eur Arch Otorhinolaryngol. 2023;280(8):3765-3771.
doi pubmed - Fortunato JE, D'Agostino RB, Lively MO. Pepsin in saliva as a biomarker for oropharyngeal reflux compared with 24-hour esophageal impedance/pH monitoring in pediatric patients. Neurogastroenterology & Motility. 2017;29(2):e12936.
doi - Mozheiko TV, Ilchenko SI, Fialkovska capital A C, Koreniuk OS. Specific features of the oral microbiome in young children with aryngopharyngeal reflux and its role the development of recurrent respiratory diseases. Wiad Lek. 2023;76(1):58-64.
doi pubmed - Gao X, Liu DG, Wang F, Zhang C, Du X, Wu JM, Wang ZG, et al. Efficacy evaluation of pepsin in laparoscopic antireflux surgery for gastroesophageal reflux disease. Technol Health Care. 2021;29(1):91-97.
doi pubmed - Orhan AI, Alkan A, Orhan K, Tezel A, Karaoglanoglu S, Oztas D. Dental caries and associated factors among Turkish children and adults: Findings from the 3rd National Oral Health Survey. Community Dent Oral Epidemiol. 2024;52(4):499-508.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
International Journal of Clinical Pediatrics is published by Elmer Press Inc.